
Summary/Abstract
Myofascial Pain Syndrome (MPS) is a common overlooked and underdiagnosed condition. MPS can evolve into fibromyalgia, and many studies focus on central mechanisms. Therefore, the purpose of this scoping review is to systematically search cross-disciplinary studies of MPS, focusing on mechanical aspects, and suggest an organic mechanism explaining how it might evolve into fibromyalgia. Systematic searches on MEDLINE, EMBASE, COCHRANE, PEDro, and medrXiv were performed, following PRISMA-ScR guidelines. 798 items included. Review suggests fascia can adapt to various states by reversibly changing biomechanical and physical properties. Trigger points, tension, and pain are a hallmark of MPS. Myofibroblasts play a role in sustained fascial tension which can propagate and is a basis for a tensegrity framework. Movement and mechanical interventions treat and prevent MPS, while living sedentarily predisposes to MPS. MPS can be seen as a pathological state of imbalance in a natural process; manifesting from inherent properties of the fascia, triggered by a disrupted biomechanical interplay. MPS might evolve into fibromyalgia through deranged myofibroblasts in connective tissue, or “fascial armoring”, which may explain pain distribution, decreased pressure/pain thresholds, occasional resolution after surgery, etc. Lifestyle is linked to pain and suffering. The mechanism of needling is suggested to be mostly mechanical.
Perspective This scoping review highlights the role of myofibroblasts in myofascial pain syndrome (MPS). MPS might evolve into fibromyalgia through “fascial armoring”. A global percutaneous needle fasciotomy that respects tensegrity principles may treat MPS/fibromyalgia more effectively. Functional somatic syndromes can be seen as one entity, perhaps sharing a common rheuma-phycho-neurological mechanism.
Introduction
Chronic pain is a major cause of morbidity and has a significant impact on quality of life.1 Myofascial pain denotes a pain arising from muscle and fascia. Commonly known as “muscle knots” myofascial pain usually arises in trigger points (TrPs) or ‘tender spots’.2,3,4 TrPs are small and sensitive areas in a contracted muscle, that spontaneously or upon compression cause pain to a distant region, known as a referred pain zone.3,4
Myofascial pain syndrome (MPS) is an entity that still lacks a clear definition. Some define it as a regional pain disorder,2 others define it on the basis of tenderness and associated painful spots.3 Nonetheless, TrPs and myofascial pain are a hallmark.2,4,5 A fundamental difficulty arises when there is no clear definition, epidemiology, pathophysiology, or diagnosis of MPS. Having no accepted definition or criteria, clearly raises issues for both diagnosis and potential studies.6-8 The purpose of this paper is to systematically search the empirical studies and components of MPS in an effort to assemble them into a suggested organic mechanism, explaining its pathophysiology and how it may evolve into fibromyalgia. Since much of the subject is still somewhat under dispute, textbooks and medical literature were added to establish a consensus on the elements of MPS.
In clinical practice MPS is often defined by multiple areas of musculoskeletal pain and tenderness associated with painful points.3 Pain is deep and aching. It may arise after trauma, overuse or sedentarism.3A study found laborers who exercise heavily are less likely to develop manifestations of MPS than sedentary workers.3 Palpation of a TrP can reproduce or accentuate the pain.4However, these findings are not unique to MPS: in a controlled study they were also present in “normal” subjects.3 Literature estimates 45% of men and 54% of women in the general population have TrPs.2,9 Estimates are 37 to 65 percent of the population have myofascial pain, which costs the united states $47 billion every year.4,10,11 MPS is one the most frequently under-diagnosed, under-treated and misunderstood sources of the ubiquitous aches and pains of humankind.4,9 However, even recently, MPS is considered by some to be fiction, or otherwise paired with psychosomatic disorders since it involves pain and has no clear pathophysiology.11-13
Although MPS and fibromyalgia are defined as separate entities, the two may co-exist or considerably overlap.2,3 They are both characterized by painful points, silent routine laboratory investigations and no systemic inflammation.2,3,4 In some patients, regionally localized MPS may seem to evolve into fibromyalgia.3 The puzzle of the mechanism of MPS and how it may develop into fibromyalgia still eludes our understanding. The marked dissociation between the estimated prevalence and burden of MPS, and the length of text on it in common medical textbooks, reflects this lack of understanding.
Studies of fibromyalgia reveal odd findings eg, complete resolution after laparoscopic surgery, and strong overlap with other conditions. Many theories exist for fibromyalgia, the most accepted and studied seems to be central sensitization, but no single theory seems to explain a wide range of empirical evidence, and the pathophysiology and etiology are still not clear. Treatments are insufficient, meanwhile patients suffer. This scoping review focuses on the organic mechanical aspects of myofascial pain with the hope it might advance our understanding of MPS and fibromyalgia and stimulate research in a less explored field.
Methods
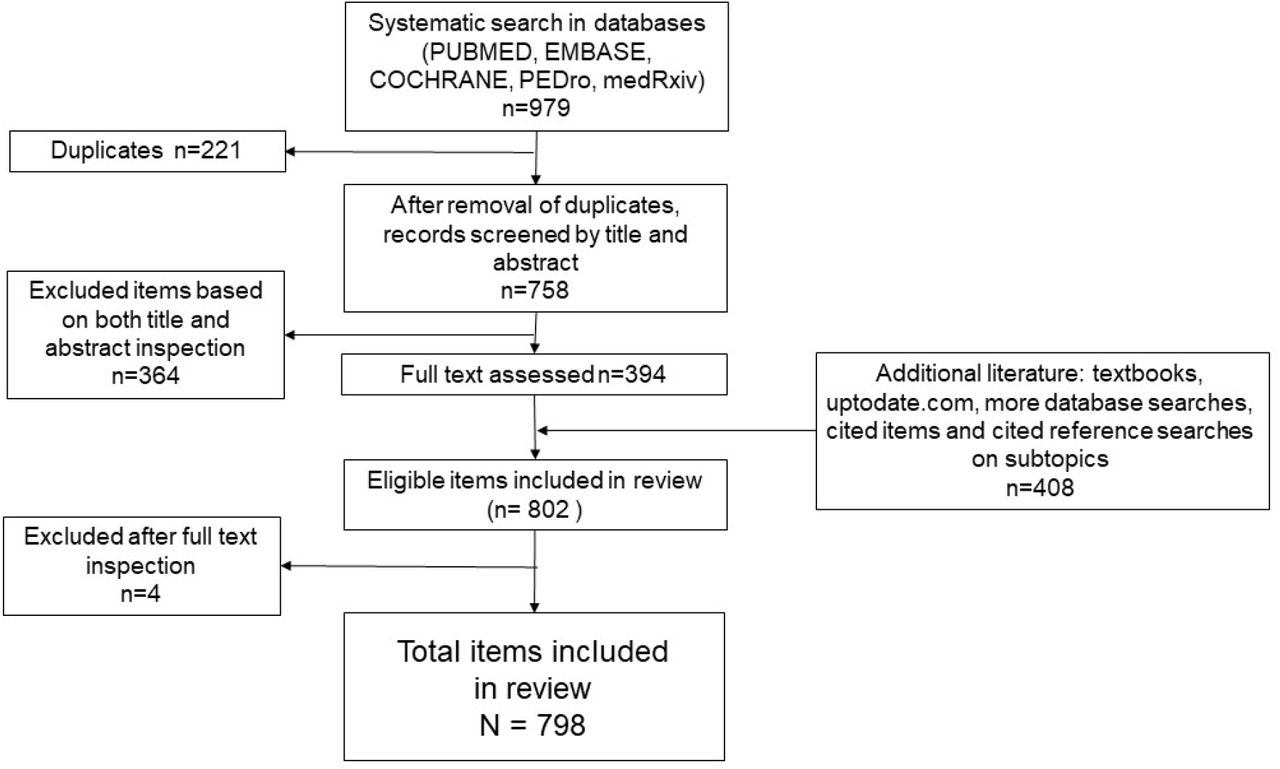
A systematic search was held for multiple combinations of keywords in multiple databases. Keywords included : “fascia tension pain”, “trigger point satellite”, “fascia stiffness pain”, “Fascia Densification”, “trigger point densification movement”, “biotensegrity”, for all fields with no time limit; and for “Risk factors myofascial pain syndrome” only for title/abstract; Systematic reviews, meta-analysis and randomized controlled trials were searched in title or abstract for “myofascial pain syndrome”, “spinal mobilization sympathetic nervous system”, “sympathetic activity induced by pain” since 2015. The databases used were National Library of Medicine PUBMED (MEDLINE), COCHRANE, EMBASE, PEDro and medRxiv. Web of science was used to find items through a cited reference search. All searches were done between September 2020 and June 2021. Only items published in English were included. This work follows PRISMA guidelines for scoping reviews. The systematic search yielded 979 items. After removal of duplicates (N=221), 758 items were screened by assessing both title and abstract. Items off topic, foreign language, and in journal ranked Q4 were excluded (N=364). For the remaining items (N=394) a full text determination of eligibility was then performed. Four items were excluded. Final number of items included in systematic search was N=390.
When side topics were encountered, literature was added to broaden scoping review via medical textbooks, www.uptodate.com and more studies from searching databases (n=408). These side topics were not searched systematically. An attempt was made to cite more than one source in such cases. Total review items: 798. Figure 1 shows the flowchart of the scoping review.

Flowchart of scoping review.
Results
A total of 798 items were included. Numbers of items by recurrent themes were: “MPS and trigger points” (n=95), “properties of fascia” (n=47), “anatomy and movement” (n=43), “nervous system” (n=31), “biotensegrity” (n=26), “myofascial pain treatment” (n=209), “myofibroblasts” (n=93), “fibromyalgia” (n=92), “reviews” (n=33), and “other” eg, somatic syndromes, stress, chronic pain, Dupuytren’s disease, plantar fasciitis (n=129). The systematic search included 127 clinical trials, 33 systematic review, and 19 meta-analysis. The findings are presented with the purpose of understanding the elements relevant to MPS and fascia, in order to assemble them and discuss a suggested mechanism of MPS and fibromyalgia. A microscopic view will set the stage for a macroscopic understanding.
Properties of fascia
General
Fascia is an important yet often misunderstood tissue in medicine. Essentially, fascia is connective tissue composed of irregularly arranged collagen fibers, distinctly unlike the regularly arranged collagen fibers found in tendons, ligaments or aponeurotic sheets.14 When connective tissue collagen is pressed, it can chondrify.15 Fascia pervasively extends from head to toe, it envelops and permeates muscles, bones, blood vessels, nerves, and viscera, composing various layers at different depths.16 Fascia supports the human body in vital functions such as posture, movement, and homeostasis,14,16-18 as well as containing various sensory receptors for proprioception, nociception, and even hormones.18 Nociception is influenced by the state of the fascia.18 This means pain can arise from changes in the connective tissue.18,19 The interconnectedness of fascia and its ability to transmit force are at the basis of its functions.18 Fascia is continuous from the trunk across the upper and lower limbs and hence has the potential to influence range of motion.18 Fascia seems to connect the distant hip and the ankles, not only anatomically, but also mechanically, supporting the concept of a myofascial continuity.18
Biophysical and mechanical functions
Fascia has properties that enable it to reversibly change its stiffness and decrease the forces of tension experienced by it. This is a mechanical ‘stress relaxation’ resulting from the viscoelasticity of fascia that expresses high or low stiffness, depending on the rate of loading. Some experimental tests demonstrate a 90% of stress relaxation achieved in about four minutes, afterwards the stress relaxation curve is near linear horizontal.20-23 Other studies observe increase in stiffness when ligaments are successively stretched, ie, strains produced by successive and identical loads decrease. They recover to baseline after a rest period. Isometrically maintained stress resulted in gradual tightening of the tissue.14
Blood vessels and nerves are interspersed in fascia, therefore, involvement of these structures due to fascial changes is commonly seen.14 It is noted a tender point in the gluteus medius can refer pain down the leg and mimic sciatica.3 Often the patient is aware of numbness or paresthesia rather than pain.9Pain is the result of a microenvironment around the nerve composed of connective tissues (eg, deep fascia, epineurium). Tissue modifications can be translated into change in nerve mobility, with a consequent decrease in the independency of the nerve from its surroundings. Altered fibrous tissue around nerves can lead to entrapments and lesions.24,25 Circulation and perfusion can also be compromised. For example, dysfunction of the posterior layer of thoracolumbar fascia has been reported as a “chronic compartment syndrome” of the paraspinal muscles.26
Hyaluronic acid
Hyaluronic acid (HA) has a key role for fascia. It is the major glycosaminoglycan of the extracellular matrix (ECM) and a major constituent of connective tissue.27 Its concentration, as well as the temperature and other physical parameters, determine the physical properties of the ECM.27-30 In fascia, HA is present within the sublayers and facilitates normal free sliding.27 Infra-red spectroscopy of viscous HA indicates water molecules can be arranged tetrahedrally almost like as in ice.29 HA interchain interactions are reversible, disaggregation occurring with an increase in pH and temperature; a gel-like to fluid-like transition occurs at 35-40 °C.29 HA solutions can express high viscosity and non-Newtonian flow properties,28 and HA’s osmotic activity is relatively high; Its stiffness occurs in part due to its long chains forming an entangled large volume network.29,30 Once viscosity increases, HA can no longer function as an effective lubricant; this increases resistance in layers with abnormal sliding.27
Fascia and movement
Fascia acts as a key player for generating movement.16 Although often a dropped prefix, fascia is part of the (fascio)musculoskeletal system. It is suggested to be able to transmit tension and affect other muscles, reflecting the direction of force vectors, and play a role in properly coordinated movements of the body.31
Sedentarism
Non-versatile movement patterns and sedentarism are an important lifestyle component for fascial changes and pain.3 A meta-analysis found that low work task variation is a risk factor for non-specific neck pain.32 Immobilization of a limb or body segment can lead to pathological changes in the connective tissue. Studies of immobilization suggest an increase in collagen and myofibroblast density as early as one week after immobilization;33 After about 4 weeks the collagen fibrils become arranged anbormally.34Regular physical activity is recommended for treatment of chronic pain and its effectiveness has been established in clinical trials for people with a variety of pain conditions.35 Proper posture and resting positions are important in preventing muscle tension.3 Pain often recurs unless appropriate exercises are prescribed.5
Tensegrity
The fact that fascia can transmit tension to a distance is a basis for a “bio-tensegrity” framework.36,37 Bio-tensegrity applies principles of tensegrity to our understanding of human movement. Tensegrity is an architectural principle. According to this, structures (or tensegrity systems) are stabilized by continuous tension with discontinuous compression.37
When the tension of fascia increases, the connective tissue can distribute the forces throughout the surrounding areas, propagating along the myofascial system.14,18 According to Wilke et al.38 fascia links the skeletal muscles, forming a body-wide network of multidirectional myofascial continuity. Cadaveric studies suggest a clinically relevant myofascial force transmission to neighboring structures in the course of muscle-fascia chains (e.g., between leg and trunk).38 A study suggests manual traction to the biceps femoris tendon results in displacement of the deep lamina of the thoracolumbar fascia up to level L5–S1.14 Acute bout of stretching of the lower limbs increases the maximal range of motion of the distant upper limbs and vice versa.18 Recent studies indicate that tightness of the gastrocnemius and hamstrings are associated with plantar fasciitis.39 Since most skeletal muscles of the human body are directly linked by connective tissue, symptoms may develop in areas distant from the point of dysfunction.40
Acceptance of the concept that a fascial tensegrity system connects the whole body is not necessary for a scientific discussion of tension spreading to other areas of muscle groups or structures. Some studies indicate that a tensegrity model might not be a true representation of the whole fasciomusculoskeletal system, and some evidence supports tensional propagation only to certain areas.41
Myofascial Pain Syndrome
There are several phenomena that accompany MPS including: trigger points (TrPs), active loci, taut bands, satellites, and the local twitch response.
Trigger points - Changes in fascia are associated with pain in TrPs and tender spots. Many patients with active (ie, painful) TrPs have other areas with the same electrophysiologic findings that are not symptomatic, called latent TrPs. Latent TrPs seem to only cause pain upon palpation, while active TrPs cause pain and symptoms both at the site palpated and referred elsewhere.2,4,9 The arising of pain is attributed to those palpable areas in the connective tissue, which seem to activate nociception.2,4
Theories of the origin of TrPs emphasize the chronic contraction associated with them or their tendency of appearing at the muscle spindle.2,9 Others suggest TrPs represent hyperactive end-plate regions.7More theories that either deny the existence of MPS or believe it represents a focal dystonia, microtrauma, or are of central nervous system origin, are also hypothesized.2,7 Critics of MPS argue that the findings seen at TrPs are simply variants of a normal physiologic finding.7 There is reason to suspect this is true: about 50% of adults have active or latent TrPs,2,9 and infants have been observed with point tenderness of the rectus abdominis muscle and colic. These both were relieved by sweeping a stream of vapocoolant, which inactivates myofascial TrPs, over the muscle.5
TrPs are extremely common. Among 224 non-specific neck pain patients, TrPs were found in all of them.9In studies in pain clinics, 74-85% of those presented to a clinic had TrPs the primary cause of their pain.9 TrPs are one of the most frequent causes of neck pain and back pain.42 The severity of symptoms caused by TrPs ranges from the agonizing, incapacitating pain caused by extremely active TrPs to the painless restriction of movement and distorted posture caused by latent TrPs.5 The influence of latent TrPs on physical function is commonly overlooked.5 Patients who had other kinds of severe pain, such as that caused by a heart attack, broken bones, or renal colic, say that the myofascial pain can be just as severe.5 Some suggest TrPs are present in up to 85% of individuals with colorectal, urological and gynecological pelvic pain syndromes, and can be responsible for many of the symptoms related to these syndromes.43 It was suggested that TrPs or myofascial tension, not exerted by external forces, can apply enough force to cause various abnormalities, including compression and entrapment of anatomical structures,44 decrease joint range of movement,7,16 influence viscera,9,45,46 lead to musculoskeletal abnormalities,47 and alter blood and lymph flow.48
Active loci - TrPs show electrical abnormalities called ‘active loci’. This is a small region in a muscle that exhibits spontaneous electrical activity (SEA), often characterized as endplate noise measured on electromyography (EMG), leading to chronic contractions.9 Although some literature does not regard TrPs as a discriminating factor for MPS, the ‘Active Locus’ seems to be a consensus.7
Taut Band - A taut band is thought to be composed of several TrPs and shows excessive endplate potential activity.9 Sustained abnormal activation of acetylcholine (Ach) is hypothesized to create an “Energy Crisis” component.9
TrP Satellite - TrP satellites are another disputed aspect of MPS. Some literature states TrPs themselves can induce motor activity (referred spasm) in other muscles.49 Illustrated by an example where pressure on a TrP in the right soleus muscle induced a strong spasm response in the right lumbar paraspinal muscles.
Pressure applied to a TrP in the long head of the triceps brachii muscle indued a strong motor unit response in the upper trapezius muscle only during the 20 seconds that pressure was being applied. This response failed to be reproduced following inactivation of the triceps TrP. It is known as a ‘satellite’ phenomenon.9,49 Moreover, it seems TrPs can spread, since an active TrP in one muscle can induce an active satellite TrP in another muscle.9,49
Various hypotheses have been suggested to explain the mechanism of MPS, among them are trigger points, non-muscular sensitization of the nervi nervorum, central nervous system, and several other theories.2,7,9,50Some relate the muscle contractions in TrPs to a myotatic (stretch) reflex evoked by fascial tension.7,9
Myofibroblasts
Fascia itself is able to actively contract. Tensional alterations are caused by contractile cells.51Myofibroblasts are present in some developing or normal adult tissues, altering tissue tension.30,51 Although most tissues exist under a mechanical tension, the same is not necessarily true of their resident cells; These are protected from the relatively massive external loads by the mechanical properties of the surrounding matrix.51 In engineering terms, this is called ‘stress-shielding’, occurring due to the matrix material that they deposit and remodel.51
Normal fibroblasts are highly sensitive to the physical stimuli. Tomasek et al. show certain changes in tissue rigidity, strain, and shear forces are mechanical cues sensed by fibroblasts that lead them to trans-differentiate into another cell phenotype.51,52 In other words, the transition from fibroblasts to myofibroblasts is influenced by mechanical stress. If subjected to mechanical tension, fibroblasts will differentiate into proto-myofibroblasts, which contain cytoplasmic actin stress fibres that terminate in fibronexus adhesion complexes.51,52 The adhesion complex bridges the myofibroblast’s internal cytoskeleton and integrins with the ECM fibronectin fibrils. This enables proto/myofibroblasts to generate contractile force in the nearby ECM by traction. The force inside the ECM is maintained over time and reinforced further by remodeling and collagen deposition.51 Functionally, this provides a mechano-transduction system, so that the force that is generated by can be transmitted to the surrounding ECM.51Increased expression of alpha smooth muscle actin (α-SMA) is directly correlated with increased force generation by myofibroblasts in a positive feedback regulation.51 A vicious cycle is suggested, in which tension facilitates TGF-β1 signaling, which induces α-SMA expression. In turn, this increases development of more tension, which upregulates TGF-β and α-SMA repeatedly.51 In short, myofibroblasts generate the mechanical conditions that enhance their contractility in a detrimental loop.51 In contrast to the reversible short-lived contraction of striated and smooth muscles, myofibroblast contractility is different: with ECM synthesis and degradation (ie, remodeling) they lead to irreversible and long contractures in a process that can be maintained for long periods of time.51 It is thought that myofibroblasts use a lockstep or ‘slip and ratchet’ mechanism, in incremental and cyclic contractile events using Rho-kinase system, and aside the myosin light chain kinase (MLCK) system.51 Once achieved, contracture shortening does not require the continuing action of myofibroblasts.51 The visible appearance of continuous tension in pathological contractures is the consequence of contraction and remodeling.51 Myofibroblasts might transmit considerably high forces.51
It is also possible that myofibroblasts can couple their activity directly to other cells like myocytes via gap junctions and act as a unite.51,53 Interestingly, if the collagen lattice is released from its points of attachment such that stress in the matrix is lost, the cells rapidly undergo isotonic contraction and subsequently lose their stress fibres and fibronexus adhesion complexes.51
Treatments for MPS
Several pharmacological and non-pharmacological treatments are suggested in literature.
Non-pharmacological:4,9,11,54-57 including manipulative therapy, vibration therapy, exercise, etc. Since it is shown that needle insertion reduces pain and SEA on EMG,58 this suggests a therapeutic role for mechanical needling.
Pharmacological: 4,9-11,54 including non-steroidal anti-inflammatory drugs, opioids, topical creams, and TrP injections.
Discussion
The first part of the discussion analyzes MPS, and the second part focuses on fibromyalgia.
Part 1 – A theoretical model for MPS
Synthesis of the data gathered in this review leads the author to the following analysis and suggested mechanism:
Etiological considerations
There are three aspects of fascial induced pain to consider, from the standpoints of physics, biomechanics, and cellular biology. These seem relevant to fascial tension, TrPs, and MPS.
The standpoint of physics relates to energy. Thermodynamically, the human body can be seen as an open system of energy, and so can the fascial system. Although energy and entropy are modulated by various factors, by nature, entropy of this system will spontaneously tend to increase. To tense the fascia energy needs to be expended. Once fascia is tense the energy can remain as potential elastic energy or change due to other modifications, for example molecular rearrangement. HA has a molecular structure that enables it to have a high degree of entropy, like an entropic “sponge”. When entropy increases it generates osmotic pressure and diffusion of fluids and other processes. Thus, when entropy of HA increases, osmotic pressure increases, and stress decays. If stimulus is not removed after this acute stressing, fascia will remain in the failure part of the stress relaxation curve and will be remodeled in this state. Although entropy goes together with osmosis and stress decay, each oscillation between different energy states will likely cause a loss of energy being a non-ideal system, for example due to friction. Fascia has hysteresis and is not a perfect “energetic spring” to oscillate between high-tension and low-tension states, ie, it dissipates energy.
Secondly, from a biomechanical standpoint the review shows that (i) simple stress decay and recovery from it is a reversible process due to elasticity of fascia; (ii) trigger points (TrPs) and myofibroblasts are found in normal individuals; TrPs are seen even in childhood and infancy, and in animals.58 (iii) fascia continuously remodels itself and HA is continuously synthesized and excreted, (iv) a sedentary lifestyle and repetitive overuse of muscles, with low variability of movements, all lead to fascial changes/fibrosis and possibly MPS; (v) exercise and proper movement relieve and prevent MPS; (vi) MPS seems to recur unless appropriate exercises are prescribed.
These suggest an underlying ongoing interplay between movement and sedentarism. Since tensional changes are reversible in fascia of normal individuals and depend on the mechanical state of the human body, this indicates fascia is meant to withstand and continuously undergo dynamic changes according to varying dynamic mechanical states. Since immobility often leads to collagen alterations, HA changes, myofibroblasts, and pain, we can see MPS as a natural consequence of the sedentary lifestyle. Resulting from the evolutionary “price” biology paid in a trade-off with chemistry when trying to “come up” with a tissue as effective, pliable, compliant and strong as the fascia. This “bargain” served us well to function effectively as an organism dominated by continuous movement. It seems that by living sedentarily, the natural disadvantages of the properties of fascia (chondrifying, HA aggregation, failure to decay, and fibrosis) manifest pathologically. Stiffness and lack of mobility of fascia has implications beyond a patient being unable to move adequately; it can affect the behavior of all cells interacting with the connective tissue matrix.16. If indeed nature designed a way to relax fascia during movements and reverse these changes it might happen through (i) dissipation of fascial energy as mentioned above; (ii) mechanical effect of movement that ruptures fascial fibers or shakes off fibers, which might explain why studies find extra-corporeal shock wave therapy to be effective for MPS (eg, Uritis et al.)54; (iii) friction between sliding layers of fascia elevating the local tissue temperature, or “warming up” myofascial tissue. Literature suggests the three-dimensional supramolecular assembly of HA breaks down progressively at 35-40 degrees celcius.29 The more viscous is HA, the more friction will act to counter viscosity; (iv) increasing clearance of HA due to increased lymph flow. Higher concentrations of HA lead to its more gel-like state, affecting the properties of the matrix. (v) pandiculation; (vi) self-aware “palpation” as a part of one’s lifestyle.
The third aspect to consider is a cellular one: induction of myofibroblast by tension and by sedentarism.33,51Chronic tension is exacerbated with more tension generated by myofibroblast smooth muscle actin fiber contractions. This makes it increasingly more difficult to maintain a relaxation. Tension is converted to HA aggregation and entropy so long as compensation along the stress relaxation curve can allow for it. Increase in HA concentration is expected to keep HA in the denser gel-like state,29,59 which would plausibly be perceived by the individual as bodily stiffness. If the values of tension reached at the stress relaxation curve plateau tend be above the value of the threshold for myofibroblast differentiation, it will be a major driver for MPS (values may vary between individuals). Biologically, the reinforcing of fascial cells with actin fibers may be the way of the body to express support of the repetitive muscular effort. Accumulation of many foci of stretching along a sensory or sympathetic nerve, due to extracellular fibers pulled from multiple directions by proto/myofibroblasts, might cause peripheral nerves to be hyperirritable chronically. This may explain why a study finds the number of active and latent TrPs is significantly and negatively associated with pressure pain thresholds (Do et al.)12. A chronic peripheral pain could contribute to a central sensitization and to changes in spinal cord pathways, though, as stated, the central mechanisms are not the focus of this review. These three dimensions seem to be relevant to fascial tension, TrPs and the etiology of MPS.
Pathophysiological considerations
Manifestation of MPS is seen in TrPs. Latent TrPs may be points that have previously nociceptively sensed tension (ie, active TrPs), for example from sedentary behavior or a ‘satellite’, and then were mechanically induced to stress shield themselves via myofibroblasts. The stress shielding does not necessarily eliminate tension (and pain) completely, thus preserving some mechanical drive for further proto/myofibroblast activity. Moreover, new myofibroblasts generate alpha smooth muscle actin (α-SMA) and contractions themselves.51 When mechanical stimuli continue, fascia remains more towards the failure part of the relaxation curve, and cells have time for stress shielding and matrix remodeling. Then, latent TrPs (via myofibroblasts) start to exert their own tension. This reinforces the abnormality. However, that tension would be more diffuse as it spreads along an intricate web of fibers (ie, stress shield), inducing more tensions, more force gradients in fascia, more foci of stretch or entrapments of nerves, and other painful TrPs further away. If mechanical tension is sufficiently reduced by shielding or by other means, myofibroblast will dedifferentiate or undergo apoptosis,51 leaving behind a remodeled fascia. Multiple iterations of the contractile cycle result in incremental and irreversible tissue contracture.60 TrPs appear on ultrasound as focal, hypoechoic regions and with reduced vibration amplitude, indicating increased stiffness.12
These dynamics may be the basis for the unexplained “metastasis” of TrPs and satellites that Quinter et al. (2015)7 refer to. When sedentary behavior continues, it feeds more tension down the cascade. The clinical manifestation would be determined not only by the amount of myofibroblasts, but by the interconnectedness of their adhesion complexes, gap junctions, and fiber-cellular networks as well. Studies suggest myo/fibroblasts form an extensive cellular network and can exhibit coordinated calcium oscillations and actively respond to mechanical stimuli.61-63 Studies suggest myo/fibroblasts have stretch activated calcium channels, and that intracellular calcium and myofibroblast contractility is mechanistically linked.60,61 Langevin et al. find evidence that leads them to a conclusion that soft tissue fibroblasts form an extensively interconnected cellular network, suggesting they may have important and so far unsuspected integrative functions at the level of the whole body.62
Activating a latent TrP is hypothesized to involve interference with the stress shield or stretch-activating myofibroblasts to rapidly contract, thus exposing the area to higher tension and initiate nociception. Eliminating a TrP seems to induce a local twitch response, which possibly signifies the neuron or muscle’s calcium driven response to a recovery from an active locus or shielded tension. Alternatively, it may be on-off “flickering” of the myotatic reflex due to nearby myofibroblast rapid MLCK contractions and their waves of calcium flux. Active loci may be a multifactorial phenomenon. For example, stress shielding (with or without gap junctions) superimposed on sympathetic activity, ie, a myotatic reflex on top of sympathetic drive. It would seem plausible to expect one to “learn to relax” or “learn to cognitively override the sympathetic aspect by focusing attention”, but not to willfully override a reflex response. The fact that muscle spindles are surrounded by a capsule of connective tissue, an area that sometimes might be palpated as a nodule (ie, TrP) suggests that if there are microscopic tensions, they might possess a sensitivity to generate more tension at the spindle (via proto/myofibroblasts), thus locking the stretch reflex to a certain degree. Locking the reflex would “turn on” an active locus in the associated muscle. To complicate the above, if electrical coupling of this structure occurs with an endplate (or non-intrafuseal fibers), via myofibroblasts, it might perpetuate an “arrhythmic” picture on EMG, with background noise, and random spikes upon myofibroblast contractions. Mechanical disruption of this structure eg, manipulative therapy, should unlock this pathology, at least partially. This might be one of the reasons for different degrees of body relaxation and the inability of some to experience it.
Notwithstanding, other factors are not excluded. Factors associated with the central nervous system could also be implicated in the genesis of MPS, as well as genetics, environmental factors, psychosocial aspects, chronic sympathetic “freeze” reaction to everyday psychological stress, etc. Based on this discussion, we might expect factors affecting fascial myofibroblasts to have potential to cause tension, pain, or even lead to MPS. For example, diet is believed to play a role in MPS,9 and studies suggest myofibroblasts are promoted by certain diets and by pesticides/herbicides.64-67 Similarly, the molecule CCN2/CTGF is suggested to play a role in development of pain due to overuse,68 and CCN2/CTGF is shown to be important in myofibroblast α-SMA synthesis.69 Applying this sort of logic, we may find more factors linking myofibroblasts to myofascial pain.70-73
It is unclear where the tipping point between a status quo of movement-sedentarism and a deranged myofibroblast activity is. It is likely multifactorial, but lifestyle seems to be a major factor. A mechanical stimulus causes differentiation to myofibroblast,51,74 some studies suggest a threshold of ∼20-24 kPa.75 Therefore, mechanical forces might be one of other possible factors contributing to MPS and myofibroblast induction. For example: sedentarism and muscle overuse,3,9,76-78 infection or inflammation,4,7 and trauma/fracture or immobilizing a casted limb.4,9,74,79,80 Since MPS is so prevalent, also common overlooked factors in a lifestyle that is not evolution-oriented may be suspected, eg, medications that are shown to both induce myofibroblasts and increase risk of myofascial pain.72,73
Symptomatologic considerations
TrPs and myofascial pain, particularly when severe, can cause various symptoms that are not limited to the fascial-muscular-skeletal system. It is suggested that the sympathetic nervous system (SNS) causes TrPs.4Reciprocally, pain and TrPs can activate the SNS.2,4 This activation may actually be due to coactivation of larger diameter mechano-sensitive afferents rather than nociceptive afferents.81,82 If the SNS is activated by paraspinal mechanical stimuli, then maybe it can be activated by muscular tension alone. If so, this may serve as a slippery slope for further TrPs, active loci and MPS. Moreover, it seems that when MPS is severe, a widespread pathology may manifest like a fasciomuscular armor under the skin (ie, “fascial armoring”). For example, immunohistochemical examination of fascia from low back pain patients demonstrates a myofibroblast density comparable to that found in “frozen shoulders”.14
People with MPS fail to relax muscles due to a mechanical reason; Myofibroblasts can synthesize α-SMA fibers, which would transform fascia into a pseudo-muscular contractile tissue. It is not necessarily innervated and can remain contracted for years.51,83 Since this tension is not innervated by voluntary control, and despite involvement of the SNS, seeing these patients as people who just “need to relax” as first line management is counterproductive. Failure to address the mechanical aspect of myofascial pain is expected to lead to a detrimental cycle of pain and over medicating (a cycle seen in studies addressing ineffective treatments)11,84-86
Finally, sedentary behavior and active lifestyle are widely emphasized in public health. However, much focus is dedicated to cardiovascular and metabolic aspects. This review sheds light on the link between lifestyle and pain and suffering. It is worth noting that the most common recommended treatment of MPS found in this literature review is mechanical, including needle insertion, movement (passive or active, breathwork and vibration), and massage/manipulative therapy. It helps treat MPS or reduce fascial related pain.2,3,4,9,11,43,54-57
Therapeutic considerations
Needling was found as a recurrent modality in literature. Needle treatment of TrPs increases pressure pain threshold.49 Three elements might explain how needling can help treat MPS; These are (I) tensegrity mindset (II) trigger points and satellites (III) myofibroblast generated tension and stress shielding.
Since needle insertion itself seems to relieve pain,87 this may indicate needling creates a focus for a mechanical tearing action on the fascia. Meaning, the tension and shear stress inside fascia would pull on the weak point of fine needle insertion over time, until the sum force vectors, or horizontal components, at that point is eliminated or needle is removed. Cutting off tension and fascial fibers is expected to cause cells to rapidly contract, and subsequently lose their stress fibres and adhesion complexes.51 If proto/myo/fibroblasts are present (as a node or a line), tearing fascia would affect the tensegrity structure. Mechanical stimuli can induce myofibroblasts stretch activated calcium channels, and calcium is coupled to contraction in these cells.60,61 After calcium influx, MLCK activity might lead to increased contractile forces and tension acutely, if they do not lose their stress fibres and adhesion complexes. If needles tear the fibers, tension will decrease. Studies observe increase or decrease in contractility and stiffness, and witness needle grasp upon mechanical stimuli.88-91 Myo/fibroblasts create tension in the attached matrix, and upon release of tension cells undergo contraction resulting in a rapid contraction of the collagen lattice.51 So, it may be that any “damage” by the needle actually allows for cutting off tensions between tense nodes in the network of (myofibroblast) TrPs and satellites. Mechanically inducing changes,88,91 and allowing for the returning of fascia to its place. If inserted deep enough, it might also free edematous fluid, HA, or other factors trapped within the layers (eg, serotonin).12,92,93 This would gently change the dynamics of the structure and the entropy (hidden tension) of the system. Upon complete freeing of tension cells undergo apoptosis with reduction of α-SMA.94 Studies indicate needling lowers myofascial stiffness as measured by shear wave elastography,95-97 suggesting a potential for a mechanical “re-alignment” of the fasciomusculoskeletal system and actual tensional release.
The more stress-shielding is present at the locus of insertion, the longer it should take for relief to happen. Stretch lesions along sensory nerves should be relieved too. This treatment acts like breaking the connections in a geodesic dome of the tensegrity model and then allowing for new healthier connections to form by natural remodeling. (The following video observations may help grasp this model)98-101 Eliminating one node is not enough in this framework, on the contrary: if done improperly, it can only add tensions to other nodes in the structure and exacerbate the general pathology. Starting the relaxation process away from the focus of pain makes sense in this framework. It slowly and progressively begins to relax the primary, secondary, tertiary etc. nodes in the satellite network, approaching the highest area of unshielded tension later and collapsing the tension in a concentric way. According to the biotensegrity model, the peripheries carry tension affecting the focus and are equally important. Li et al. state that currently available needle delivery systems deform and move soft tissue and organs.102 This may suggest that inserting a needle causes windup of connective tissue and modulation of the fascial network based on internal forces. Alignment of the system should be done properly.
The question is: What is properly? What is proper needling? Where, in which order, depth and time, is best for which symptom? Studies suggest needling affects facia at the point of insertion and at a distance.91,103-105 How fast should the fascia be released? Indeed, it would be beneficial if we could monitor the mechanical state of fascia by palpation. By releasing the tension properly, the tissues can return to their healthy alignment without other areas exerting pulling forces. Following the “damage” of needling, the fascia will regenerate via myo/fibroblasts matching the bio-mechanical state. Evidence suggests that fascia regenerates within approximately 3-24 months after fasciectomy/fasciotomy.106,107 In fact, it is unlikely that tearing the fascia (if done properly) will seriously compromise physiology as this would have manifested as a complication after every invasive surgical operation. New extracellular fiber deposition will be based on optimized structural conformation.22Some may say inserting several needles subcutaneously sounds like a surgical intervention of the fascia. A gross illustration of this framework can be found in the supplementary material (Figure 2).




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
a) Illustration to assist the reader in imagining a healthy “geodesic dome” connected by spandex sheets (fascia)
With permission from PACIFIC DOMES Inc. www.eventdome.wordpress.com/
b) Normal external strain applied will tense the fascia and distribute the tension through the network of nodes.
With permission from Dome guys international www.domeguys.com
c) Chronic over-strain causes pathological changes in fascia or changes of myofibroblast and smooth muscle fibers inside the fascia. The fascia fails to distribute forces properly and keep the integrity of the structure. Structures on the dome and inside the dome are affected.
With permission from PACIFIC DOMES Inc www.pacificdomes.com
d) After ‘re-setting’ the system with needling or other techniques: “regeneration and growth of new connections over time should be determined by natural forces and pullies”. 22New areas in the fascia serve as points of focus for changes and realignment. Structures can relax and return to the minimum energy state. Fascia is always subjected to remodeling pressures and responds to the local mechanical state. However, if spatial deposition of fibers is altered with respect to physiological conditions, the rebuilding will be pathological. 22Mobilization encourages correct healing in order to avoid formation of fibrosis. 22
Taken by Jim Bourg, with permission from REUTERS News Agency.
Examples of these principles may have transpired in several studies. Three findings are briefly presented as follows. A study of 37 patients who were all diagnosed with plantar fasciitis and all had been treated with corticosteroid injection into the calcaneal origin of the fascia.108 All had a presumptive diagnosis of plantar fascia rupture. 30% described a sudden tearing in the heel, while the rest had a gradual change in symptoms. Most of the patients had relief of the original heel pain, but it had been replaced by a variety of new problems, including dorsal and lateral midfoot pain, swelling, foot weakness, metatarsal pain, and even metatarsal fracture. In all 37 patients there was a palpable diminution and footprints showing flattening of involved arch. MRI showed fascial attenuation. The study’s author concluded that plantar fascia rupture had occurred. The majority had resolution of the new symptoms within 12 months. In the rest, symptoms remained.108
A second study encountered the same enigma: 68% of patients with plantar fasciitis had a sudden rupture associated with a corticosteroid injection. Although it relieved the original pain, these patients developed new problems: arch or midfoot strain, lateral plantar nerve dysfunction, hammertoe deformity, and stress fracture.47
These examples might suggest there is room for a more sophisticated strategy in treating the fascia instead of simply aiming and firing at the pain. Maybe this should be interpreted not as an adverse event, but as a testimony that the treatment modality undermines the tensegrity system. Conceivably, behind this is a release of fascia in an area of very high tension, causing too drastic of a change in the tensegrity structure, instead of approaching this tension gradually. A sudden change might shift the forces to other areas and exacerbate the imbalances,109 perhaps sufficient to cause bone fracture. Moreover, it was found that steroid injection decreases fibromatosis, fibrosis, and myofibroblasts in adhesive capsulitis,110suggesting injection to the plantar fascia has potential to affect myofibroblast generated tensegrity forces.
The third finding that might be interpreted under these principles, is the phenomena of: “following a tooth extraction, a pain behind the ear and on the side of the face in the day or so prior to facial weakness often constitute the earliest symptom of Bell’s palsy.”3 (Kasper et al. 2018, p222-223). Guided with a tensegrity mindset, this may suggest a relationship in the “geodesic” face: a pain develops behind the ear possibly as a “reciprocal” point for tension in the jaw, which happens to be near the emergence of the facial and trigeminal nerves from the skull. This is a reasonably susceptible area with curved bones to serve as a focus for tension. Of course, it does not necessarily mean that releasing tension from around the mastoid process is the key to preventing the complication. Tensegrity domes are made of many nodes, and “to change a node is to change the dome”. Therefore, pain behind the ear is first and foremost an indication of extreme tension, and only then pain. A tension like every other myofascial tension, eg, plantar fasciitis. However, this pain is located in a dermatome of a cervical root: which is a distant nerve and is unlikely to be directly injured by tooth extraction. A sudden intervention in the face probably emulates the same action as a calcaneal injection. If high tension is present (for example a temporomandibular tension seen in up to 25% of the population)2 it will have the same potential energy to damage structures in the face, as implied by a metatarsal fracture. In the face it seems to cause a palsy of a nerve, similar to the foot. The degree of damage is modulated by the degree of the hidden energy.109 If correct, this means two possibilities present themselves: either this palsy is not a Bell’s palsy, or a Bell’s palsy is not idiopathic. In any case, it highlights the instrumental importance of gentle and progressive release of fascia in a proper way. Therefore, “not feeling much” may be a good thing when needling fascia. In fact, we can predict sometimes pain might worsen at first, reflecting a non-ideal modulation of force vectors. Less pain might also lead to better compliance from patients. Research has yet to establish empirically if fascial release prior to (or even after) tooth extraction, can affect the rates of this palsy. Modulation of tensegrity vectors may be a factor in reported cases where (i) treatment of Dupuytren’s disease leads to Boutonniere deformity,111 (ii) carpal tunnel release increases risk of trigger finger;112,113 (iii) treating the elbow for tennis elbow requires a supposedly unrelated shoulder arthroscopic decompression,114 (iv) simultaneous bilateral digital flexor rupture occur;115 or (v) spine surgery leads to compartment syndrome of the foot.116 It seems plausible since fascia is a system. Fascia appears to connect the distant hip and ankle joints, not only anatomically, but also mechanically, supporting the concept of myofascial connectivity.18 Most skeletal muscles of the human body are directly linked by connective tissue.40 Acute bout of stretching of the lower limbs increases the maximal range of motion of the distant upper limbs and vice versa.18 Fascia is continuous from the trunk across the upper and lower limbs,18 and because of the direct morphologic relation of the hamstrings and low back region, relieving tension of the posterior thigh muscles could be a conceivable approach to alleviate back pain.117
In conclusion, under the framework of tensegrity, it might be logical to first needle the dorsal foot and foreleg in plantar fasciitis, for example, assuming connective tissue is pulling the plantar fascia (ie, weak link in the tensegrity structure) and causing pain. Therefore, aiming to primarily treat the underlying tensional abnormality of fascia, and through this improving the symptoms of pain. Actually, it seems a TrP with severe localized pain may not be the source of pathological tension because myofibroblasts stress shield their area from tension. Tension is likely to focus more near hard and angled surfaces that have sharp force-gradients; initially generating active TrPs (if a nerve is there to experience this) that have yet to sufficiently stress-shield themselves with a fiber web. By this rationale we may expect points to be concentrated more in areas of fascia adjacent to solid or bony edges (spine, face, pelvis, chest, shoulders, knees, periosteum, perineurium, etc.). Tension will be present,118,119 but pain depends on the degree of sensory nerve involvement.120,121 This understanding may put MPS and fibromyalgia on the spectrum of a common mechanism; whereby a more widespread pain and tenderness appears, at least in part, perhaps due to an ‘archipelagos’ of stress-shielded points and taut-bands that generate and mask extreme tension. If true, a severe manifestation of this might be described by some as equivalent to a sort of mild to moderate chronic compartment syndrome of the whole body. Which may explain why “MPS” can “develop” into “fibromyalgia”, at least in a subset of patients. A biological translation to this might be: myofibroblast start affecting the body in a generalized MPS cascade, possibly with a reciprocal central sensitization. Also, it may be part of the explanation to why these pain syndromes are epidemiologically so closely associated with each other (as observed in population studies),122,123 why significant overlap is seen between them (reflecting anatomical overlap of involved fascia), why fibromyalgia tender points seem to distribute more near bone protrusions, why a study finds fibromyalgia symptoms and neuropathic pain correlate with tender point count (Amris et al. 2010)121, and why mechanically puncturing their fascia recurs in literature as an empirical treatment option for them. It can also help explain histological and clinical evidence indicating a picture of widespread non-severe chronic ischemia. Studies of fibromyalgia observe various organic abnormalities,124-141 which might support this framework.
Part 2 - Considering fibromyalgia as an entity of compression
Cardiovascular findings
Studies show tissue stiffness is significantly increased around TrPs,142 and blood vessels near TrPs have retrograde flow in diastole, indicating a highly resistive vascular bed.138 A global compression might explain a few findings that will be mentioned here briefly. Various abnormalities in fibromyalgia suggest an underlying widespread organic pathology that impairs perfusion throughout the vascular system. Capillary microscopy studies of fibromyalgia show fewer capillaries in the nail fold and significantly more capillary dilatations and irregular formations than the healthy controls. The peripheral blood flow in fibromyalgia patients was much less than in healthy controls.128 This suggests that functional disturbances are present in fibromyalgia patients.128 While one study shows a decrease in transcapillary permeability in fibromyalgia patients,129a few studies find abnormalities in the arterial system as well.143,144Findings from a study of biopsies in fibromyalgia cases without obvious muscle trauma indicate definite but nonspecific muscle changes which are suspected to be secondary to “chronic muscle spasm and ischemia of unknown etiology”.124 Katz et al. find muscle pressure is substantially higher in patients with fibromyalgia with a mean value of 33.48 mmHg.145 Only 2 of 108 patients had muscle pressure of less than 23 mmHg. The mean pressure in rheumatic disease controls was 12.23 mmHg. The burden of the pressure abnormality may help explain the diffuse muscle pain of fibromyalgia and may be an intrinsic feature of fibromyalgia.145 Therefore, fibromyalgia as a disorder of exclusively central pain processing should be revisited.145 This substantially higher muscle pressures is in agreement with the analogy of “a sort of mild to moderate global chronic compartment syndrome” and may explain why anxiolytics and muscle relaxants do not work very effectively with this entity. At the end of arterioles, mean pressure is approximately 30 mmHg, and then decreases further in capillaries and venules.146 Chronic intramuscular pressure of 33.48 ± 5.90 mmHg may reflect an abnormality that ultimately affects starling forces significantly, as well as the pressure gradient along arterioles, capillaries, and venules. Therapeutically, reduction of muscle pressure may change the clinical picture substantially.145 If myofibroblasts are indeed the generator of tension, then abnormal muscle pressure should be reduced by releasing the fascia, according to the “fascial armoring” model, since it is currently not a psychologically generated contraction. Shear wave speed of latent TrPs and adjacent tissue in the infraspinatus is elevated compared to controls and is associated with increased muscle stiffness.142 A study of frozen shoulder finds large numbers of capillaries and venules in the subsynovium of frozen shoulder samples compared with the controls.19 If fascial compression impedes starling forces and causes low-grade ischemia, it might be biologically expected that the body will secrete factors that increase total number of capillaries and venules. Such a biological response would lower total venule resistance via parallel resistance and re-establish a pressure gradient in the vessels.
Stiffness, Pain, and the Spine
Other body structures are also involved. Perez-Ruiz et al. find high rates of carpal tunnel syndrome in fibromyalgia,147 and (fascio)musculoskeletal involvement is prevalent: stiffness is a very common complaint.148,149 A survey of 2,596 fibromyalgia patients finds patients ranked the intensity of their pain lower than the intensity of morning stiffness.148 Considering central sensitization as a sole mechanism raises several questions: why is morning stiffness so commonly reported among fibromyalgia patients, and even ranked higher than pain? Is it simply because of sensitivity, anxiety, and physical inactivity? Does central sensitization occur only in certain sensory tracts like pressure, proprioception, and pain? There seem to be little to no report of extreme sensation of vibration, for example. Is central sensitization random or is there a pattern? Painful points seem to distribute in the same topography in different individuals. However, if the localization of pain and hyperalgesia is not random, why can sensitivity appear in almost any area in the body? Why are these areas not correlated with the homunculus? And what is special about the occiput, second costochondral junctions, knee pad, and two centimeters distal to the lateral epicondyle (Described by Kasper et al. 2018; p2637)3? Sugawara et al.150 suggest mechanical compression of the dorsal root ganglion (DRG) by a mechanical stimulus lowers the threshold needed to evoke a response and causes action potentials to be fired.150 Action potentials that may even persist after the removal of the stimulus and high mechanical sensitivity are suggested by this (in vitro) study. More in vivo and in vitro studies suggest the same.151-153 It is plausible that pulling would have a similar effect.
Wang et al. find a bidirectional association between fibromyalgia and gastroesophageal reflux disease (GERD).154 Trying to explain this without a mechanical peripheral element seems difficult. How do current theories explain this bidirectional linkage? Perhaps we should give fibromyalgia more mechanical credit.
This entity, if it is what it seems, would probably affect gastroesophageal pressures and relaxations, and theoretically, mechanically compress the paraspinal and intervertebral fascia and its contents eg, DRG and/or the sympathetic chain against a vertebral body. If compression has a similar effect on the sympathetic ganglion/trunk as it does on the DRG, it might add a component of sympathetic abnormalities. Indeed, studies suggest mechanical pressure on the sympathetic trunk due to osteophytes can cause various abnormalities.155 Studies suggest para-articular fibrosis in the spine can involve neural structures and cause tethering and irritation of nerves.156 A compressive factor can explain decreased pressure/pain thresholds and explain why they happen to be strongly associated with autonomic abnormalities. It also implies these abnormalities can be illusive and reversible in certain conditions. By the same rationale we might expect higher incidence of obstructive sleep apnea even after correcting for body mass index.
Considering multiple theories
More studies indicate fibromyalgia may include easy bruising,149,157 hair-loss,149 reduced skin innervation,158 tingling, creeping or crawling sensations,159 reduced fecundity or infertility,160,161urinary urgency,159 changes in bowel habits,3 decreased optic disk perfusion,127 dry eyes, 159 functional voice disorders (including muscle tension dysphonia),162wheezing,149, seizures,149 impaired cognition,149 and Raynaud’s phenomenon.163 Can central sensitization and neuroplastic pain circuits alone be the explanation of all these manifestations? Do psychosocial theories or somatization explain these? No single theory seems to fully account for fibromyalgia. For example:
If it is sympathetic hyperactivity, why does it cause wheezing?
If it is sympathetic-parasympathetic dysregulation, why is postural hypotension not in the diagnostic criteria, and why is it strongly associated with sicca but lacks reports of chronic sialorrhea?
If it is inflammatory or autoimmune, where are the inflammatory markers and why does it respond to tricyclic antidepressants? Moreover, what underlies the close association of acquired immunodeficiency syndrome,164 and why does a study find placebo has a better outcome than steroids as a treatment for fibromyalgia?165 A low-grade neuroinflammation might occur sub-clinically, but what drives it? The full cytokine profile of MPS and fibroblasts is not covered in this review, however, some studies suggest chronic myofascial pain is associated with, or causes, elevation of cytokines and inflammatory mediators, fibroblast growth factors, serum reactive oxygen species, and neuroendocrine signaling.19,166-168 However, not all studies find the same.168
Evidence for the input of psychosocial factors and stress in the pathogenesis of fibromyalgia is suggested in studies.149 If it is caused by stress and low mood or due to childhood experiences of distress, how does it reduce skin innervation and why selective serotonin reuptake inhibitors (SSRIs) or anxiolytics are not the first line treatment?
Central sensitization is the most accepted explanation. Why should exercise (or movement) be the cornerstone of treatment and how is Ehlers Danlos/hypermobility syndrome related to it? The pathogenesis of peripheral and/or central nervous system changes in chronic widespread pain (CWP) is unclear, though, peripheral soft tissue changes are implicated.169 Some evidence from interventions that attenuate tonic peripheral nociceptive impulses in patients with CWP syndromes like fibromyalgia suggest that overall fibromyalgia pain is dependent on peripheral input.169Allodynia and hyperalgesia can be improved or abolished by removal of peripheral impulse input.169 Central disinhibition is also hypothesized. However, this mechanism also depends on tonic impulse input, even if only inadequately inhibited. Thus, a promising approach to understanding CWP is to determine whether abnormal activity of receptors in deep tissues is part of the manifestation and maintenance of this condition.169 Perhaps the relationship between fibromyalgia and hypermobility syndrome has to do with changes in extracellular matrix properties that induce myofibroblasts, thus initiating a widespread MPS cascade? Studies of patients with Ehler-Danlos/hypermobility syndrome find up to 80-100% have CWP and evidence supports a close association between hypermobility syndrome and fibromyalgia.170,171 Of all associations with fibromyalgia, Ehlers-Danlos/hypermobility syndrome is one of the closest, perhaps even closer than depression. Why? Studies of Hypermobility syndrome find cells express an increased transition to the myofibroblast phenotype.172,173 A study suggests changes of collagen microarchitecture regulate myofibroblast differentiation and fibrosis independent of collagen quantity and bulk stiffness by locally modulating cellular mechanosignaling.174 The indistinguishable phenotype of myofibroblasts identified in hypermobility spectrum disorders resembles an inflammatory-like condition, which correlates well with the systemic phenotype of patients.172 These findings suggest that these multisystemic disorders might be part of a phenotypic continuum rather than representing distinct clinical entities.172 According to this discussion, widespread induction of myofibroblasts suggests a possibility for generalized peripheral pain caused by generalized tension and compression. Under this framework, the link between fibromyalgia and a variant of collagen is somewhat anticipated based on fascial biology.
There are those who suggest fibromyalgia is not a real entity or that it is caused by sleep disturbances. However, the relatively modest efficacy of antipsychotics and/or melatonin and/or z-drugs implies it is probably neither an imaginary hallucination nor due to lack of sleep.
Noteworthy, two parallel mechanisms (or more) might be at work and are not necessarily incompatible with each other. Gupta et al. 2007 studied CWP in somatising individuals. They conclude that while a high tender point count is associated with the onset of new CWP, a low pain threshold at baseline is not.175 With our new view of MPS it is logical, since tender point count would be a marker for a fascial tensional pathology, leading to widespread pain and a lower pain threshold later.
Does “fascial armoring” fill in the gaps regarding some of these anomalies? If affecting the trunk, a constrictive element might be able to impair lung function and contribute to wheezing. If involving the cervical fascia and face, it might affect salivary ducts/glands, affecting salivation. A link to phenomena like seizures/pseudoseizures will be suggested below when mentioning the myodural bridge. Interestingly, studies suggest tricyclic antidepressants can downregulate myofibroblasts and ACTA2 gene expression,176,177 and some SSRIs may actually enhance them;178 it seems gp120 enhances them too.71,179 We could similarly predict that the pathogen Borrelia may lead to connective tissue changes and increase myofibroblast activity. Thus, resulting in an infectious version of fibromyalgia with or without pronounced inflammation. Indeed, Borrelia and fibroblast co-cultures show a significant induction of type I collagen mRNA after 2 days (p < 0.02) and a significant upregulation of mRNA expression of TGF-β (p < 0.01).180 Since TGF-β is a cardinal signal for myofibroblast α-SMA synthesis, this may explain why of all infections, Lyme disease is strongly associated with fibromyalgia. Due to the stark similarity to fibromyalgia, such events can be expected in connective tissue in “post COVID-19 syndrome”. Unudurthi et al. suggest the infiltration of neutrophils, macrophages and CD4+ T lymphocytes in COVID-19 patients can promote the activation of fibroblasts to myofibroblasts in heart.181
Some research methods investigating fibromyalgia assume there is no peripheral organic lesion that causes the pain experienced. Magnetic resonance studies of the brain do not necessarily distinguish between a purely neuroplastic pain and one arising from the periphery. Therefore, it would benefit our understanding of central mechanisms if studies had a tool to identify whether mechanical fascial pain due to myofibroblasts is present in the individuals being studied, and if the pain measured arises from the periphery or not.
Some research suggests that in fibromyalgia, a global pathology involving tryptophan might come at the expense of other serotonergic operations such as in the brain.182 A mechanosensitive effect can trigger serotonin release from enterochromaffin and neuroendocrine cells.183,184 Serotonin is involved in the cellular signaling of connective tissue cells.185,186 Various studies of fibromyalgia patients indicate an elevated level of serotonin in myofascial tissue and platelets, while a decreased level of tryptophan and its derivatives, serotonin and kynurenine, is observed in the blood and/or brain.187-193 Some fibromyalgia patients are found to have decreased rate of transport of tryptophan across the blood brain barrier.181 Might a peripheral depletion of biogenic amine metabolites play a part in the association between fibromyalgia and mood disorders?
Complete resolution of fibromyalgia
Several studies point to a peculiar phenomenon. Saber et al.194 witness high rates of complete resolution of fibromyalgia following laparoscopic Roux-en-Y surgery. By which mechanism does a longstanding central sensitization completely resolve following abdominal surgery? Could this be a result of an overlooked fasciotomy? The authors of that study suggest resolution may be due to weight loss, increased physical activity, and lifestyle changes. However, this idea does not align with findings of Adkisson et al.195. They studied the effect of parathyroidectomy on fibromyalgia among 76 patients diagnosed by specialist or primary care physician. Findings show that 21 percent of fibromyalgia patients discontinue all fibromyalgia drug medications after parathyroidectomy, and 89 percent have relief of one or more fibromyalgia symptoms postoperatively. These changes occurring as early as one week after neck surgery.195 Yet, 11% of patients had no improvement in symptoms at all. The authors explain the complete resolution in 21 percent by suggesting a misdiagnosis, ie, these patients actually did not have fibromyalgia in the first place. However, if this was true, we might expect these individuals to cluster more towards the group not diagnosed by a specialist. Surprisingly, 23 out of 76 were diagnosed by a rheumatologist, out of them 96% had symptom improvement, and 70% were able to discontinue all medications after parathyroidectomy. Uncannily, 88% of those who did not experience any improvement in fibromyalgia symptoms were diagnosed by a primary care physician (p<0·05). The statistics suggest some non-random phenomenon caused a bimodal-like distribution. In light of this study, it might be hypothesized fibromyalgia is related to a parathyroid cause. However, a similar enigma is found with irritable bowel syndrome (IBS), a functional disorder with no definite organic findings and closely associated (or overlaps) with fibromyalgia. Some suggest fibromyalgia and IBS are actually the same entity.149 IBS is shown to be relieved below Rome II criteria in 80 percent of patients after laparoscopic fundoplication for GERD.196 Looking for a common denominator one can hypothesize that relief is achieved due to intense pain exposure and general anesthesia that resets the brain circuits, somewhat similar to electroconvulsive therapy combining gate control. But it does not align with findings that tonsillectomy increases risk of IBS,197 that umbilical hernia repair surgery seems to predispose to IBS,198, and that patients with fibromyalgia have a higher incidence of suffering IBS after appendectomies.199 Moreover, hysterectomy, with or without oophorectomy, seems to worsen fibromyalgia.200
Oddly, why does the location and type of surgery seem to regulate the positive or negative impact on these conditions? Indeed, it was suggested in this literature review that MPS/TrPs can cause chronic changes in bowel habits. Should we suspect that in these associated disorders, the connecting motif is connective tissue? This may imply that the location of the surgery has different effects on fascia, even remotely, due to- and regulated by-tensegrity forces. The lateral raphe and common tendon of the transversus abdominis are suggested to form connections between, and transfer tensions between, the abdomen and the paraspinal muscles and sheath.14,201 This can explain how laparoscopy might release a compression on the DRG. Interestingly, this would mean the clustering of patients experiencing benefit post-parathyroidectomy towards the group diagnosed by a rheumatologist, and those not experiencing benefit towards the group diagnosed by primary care physician, isn’t due to misdiagnosis but precisely because rheumatologist really identify those with fibromyalgia statistically significantly more accurately.
Compression vs. global percutaneous needle fasciotomy
Studies show obesity induced connective tissue fibrosis is dependent on mechanosensitive signaling.202Fibrosis, via myofibroblasts, alters subcutaneous tissue plasticity and increases connective tissue rigidity and stiffness.202 Thus, obesity might be associated with fibromyalgia by way of mechanically compressing fascia with higher forces. A study in vivo suggests applying tension on skin induces myofibroblasts.74 Therefore, by this same rationale we might expect a sedentary individual that tends to wear tight clothes and accessories that mechanically compress fascia to be at higher risk for this pathology over time. It was shown the association between a higher incidence of fibromyalgia and estrogen is unlikely.194,203 Estrogen is suggested to inhibit myofibroblast differentiation and is associated with lower fascial stiffness,204-207 and hormonal contraceptives may reduce the risk of fibromyalgia in women.208Some suggest fibromyalgia may be linked to menopause.209 This could be part of the explanation of why fibromyalgia is more prevalent in certain females. Other studies show that applying a splint or mechanical tension induces myofibroblasts,80 and ponytails/hijabs/braziers appear to cause myofascial pain.210-214 This phenomenology appears to be similar, or the same as the old practice of applying bandages to treat “rheumatism” patients (William Balfour 1815),215 meaning: modulation of the tensegrity structure and/or induction of stress shielding but failing to resolve overall tension (eg, the case of Mrs. M. p179-180). Interestingly, experimental models of restraint stress apply mechanical restraint and/or limit movements.216-220 These models seem to induce mechanical and cold allodynia, depression and anxiety like behavior, gut dysmotility, and other phenomena.216-220 Thus, one might wonder what is the pluripotent entity that restraint stress tries to model? Is it only psychological stress?
In any case, perhaps a treatment or prophylaxis that applies multiple needles in different areas of the tensegrity system, could be utilized as a global percutaneous needle fasciotomy. The theoretical end purpose this treatment would be to passively lower global fascial stiffness beneath the threshold necessary for myofibroblasts activity, and slowly experience a tensional collapse. Literature indicates fascia of patients with fibromyalgia or myofascial pain measures statistically significantly higher on shear wave elastography,221,222and that needling reduces pain.223-227 Studies also suggest needling significantly lowers the shear modulus of myofascial tissue as measured by elastography (p < 0·01),95causes mechanical changes at the point of insertion and at a distance,91,102, causes windup of the connective tissue,105 and improves perfusion to the area.228 A systematic review suggests that needling improves pain and stiffness in people with fibromyalgia and MPS.225,226,229 Also supporting this modality’s capability of improving perfusion, is a study showing infiltration of TrPs reduces symptoms of intermittent claudication.230 Symptomatically, a person constantly exerting effort against such forces of a suffocating fascia would likely feel chronic fatigue and soreness, while accumulating nociceptive substances in muscles in a chronically tonic body; and active loci induced “energy crises”. With regards to active loci, it is possible the cell has its own ways to oppose this abnormality. When synaptic neuromuscular activity is maintained over time, an aggregated form of amyloid beta is seen to interfere with Ach release ex vivo.231 One adopting this biological ethos should not be surprised if amyloid beta has some role in “fascial armoring”, because studies suggest amyloid beta, and the cytoskeletal protein tau, are affected by- or compensate for-mechanical stress.232-236
At least we might want to exclude an organic fascial cause before perceiving these cases as purely psycho-functional disorders, even if the mechanism is still unclear. Is there enough empirical evidence to recognize MPS and fibromyalgia as honorable organic diseases, like any other? Medicine is used to entities that are either immune related, infectious, malignant, endocrine, metabolic, genetic, cardiovascular, neurologic, traumatic or toxic, but not familiar with many mechanical ones. If medicine overlooked another system causing pain besides fascia, like integumentary or skeletal, it would probably lead to overlying on psychology to explain it. It is difficult to explain all the empirical evidence relating to fibromyalgia (eg, association with hypermobility syndrome or the complete resolution soon after surgery) while relying on central sensitization and stress or somatization alone. Therefore, investigating a link between fibromyalgia and a peripheral mechanical process might benefit our understanding.
The enthusiast of the principle of Occam’s razor (ie, minimize multiplication of entities) might consider seeing other functional entities that are known to be associated with pluripotent TrPs,2,4,12,43,237,238as “MPS”/”fibromyalgia” that is localized to certain anatomical areas; coupled with the reciprocal central nervous system changes. “Kelley’s textbook of rheumatology” and others suggest functional somatic syndromes to be on a continuum of one entity with fibromyalgia.122,149,162 Myofascial TrPs reproduce the pain pattern of fibromyalgia and are related to widespread mechanical hypersensitivity.239 In addition, MPS and fibromyalgia are suggested to be two sides of the same coin.2,240 Etymology does not necessarily reflect pathophysiology, but the term “fibromyalgia syndrome” basically carries the same meaning as “myofascial pain syndrome” but in Greek. The analysis based on this scoping review offers one mechanical aspect as a part of a common rheumapsychoneurological mechanism.
Final note
Based on this review, it seems that fascia is an intelligent and sophisticated tissue network, at least like any other tissue network we know. It is shown myo/fibroblasts have gap junctions that can couple and directly communicate with each other (Xu et al. 2021)241 and with other types of cells (with heart,242 hair follicles,243 cancer cells,244 etc.).51,245-249 These can contract as a unit or in patterns,250,251 affecting the organ’s functionality.53,252-259 If this theoretical model of myofibroblast generated tensegrity tension is verified empirically, it might be worth further exploring the possibility that they can couple in vivo (directly, or indirectly through myocytes/glial cells) to nerves. Studies suggest the meninges might be coupled to the cerebral cortex to form one large network with myo/fibroblsts.260-263 The myodural bridge connects the extracranial occipital fascia with the dura.264 Myo/fibroblasts seem to form a body-wide cellular network; They can respond to mechanical cues and exhibit spontaneous calcium oscillations and synchronized contractions,62,249-251,258,265-267 and fibroblast themselves can induce contracture through actin beta and gamma pathways.268 We could consider the hypothetical possibility that this dynamic body-wide mechanoelectrical network of cells and fibers has an overlooked interplay with the network of the human nervous system. This idea might disguise some of the pathophysiology of self-psychosomatics and potentially help us understand why a remarkable 17 percent of primary care patients are diagnosed with somatic symptom disorder (SSD) (defined in studies as at least four or more unexplained symptoms)269, why tender point counts are predictors of CWP in somatising subjects,175 and why SSD is associated or overlaps with fibromyalgia. There are those who believe tensions in the body are closely linked to our emotions and personality (eg, W. Reich and A. Lowen).170,171 We know biology does not separate itself into different medical specialties like we do occupationally.
Lastly, if myofibroblast can engulf their surroundings,272 and in certain conditions are able to present antigens via MHC class II to T cells,273-276 then we might want to examine the potential role of myo/fibroblast fascial networks (or differentiated/somatic-mutated clone populations) in immune related conditions. Empirics suggest a link between fibromyalgia and other rheumatological disorders, and apparently, a study from 1990 of 20 patients with fibromyalgia suggests the majority have anti smooth muscle antibodies.277,278
On a spectrum of “normality” we may all have “MPS” to some extent, technically speaking. It seems to be a question of how much we have and how much it affects our life. A tradeoff is still being made, no longer by biology but by humans. Not regarding the molecular design of fascia, but it is an ongoing tradeoff between not moving and moving. As it seems to be a natural condition worsened by an un-natural lifestyle, we may say living sedentarily misses our evolutionary target (ie, a “biological sin”). It is interesting a study by Younger et al. finds patients with myofascial pain have changes in grey matter in the hippocampus, anterior insula, and cingulate cortex, among several areas:279 Forgetting our evolutionary purpose seems to impair our memory, while cognitive detachment from our body-awareness seems to impair our cognition, and because the biogenic amine metabolites are low, the above suggests a lifestyle with scarcity of movement will rarely make us blissful. Looking through the given titles of these entities, we might find what we most want to find where we least want to look. A body that cannot move with total freedom will hold a mind that is seldom totally free of dis-ease. This aligns with the notion that the body and the mind are accepted to be one being. Just as we can say music is a “collection of noises” or a “divine melody”, so may we say MPS is “pulled muscles” or a “fascinating disorder of the fascia”. Assembling these conclusions and concepts to creatively connect this medical puzzle is the easier part of this not so easy effort. The major challenge now being the research needed to verify or disprove them, and moving forward with evidence on this topic while moving ourselves…
Limitations
The main limitation of this scoping review is that a sole researcher evaluated the studies. It is based on other empirical studies where some are in vitro studies, as mentioned in parts of the discussion. Being a scoping review, although a broad searching strategy was applied, not every topic was searched systematically. A systematic search was done for several main key phrases, in five databases. Systematically searching for relevant side topics (ie, topics not defined in the key phrases) was not feasible, unfortunately. For side topics, an attempt to find a reliable source of information, like a textbook or study (or both), was the strategy to gather information. In such cases an attempt to cite more than one study was made. Worth noting, no on topic studies were found when searching “fibromyalgia myofibroblast” or “fibromyalgia alpha smooth muscle actin”. The cytokine profile and the topic of vitamin D in fibromyalgia was not discussed even though a study finds vitamin D might play a role in myofibroblast attenuation or de-differentiation.280
Contributions: this work was done by the sole researcher and author of this manuscript including conception, organization, literature review, integration of information, findings analysis, manuscript preparation and writing.
Data Availability
All data is available in the manuscript file
Conflict of interest
The author declares no conflict of interests.
Funding
none
Acknowledgements
Professor Pnina Ohanna Plaut for assisting with methodology and editing. Dr. Bronya Gorney for assisting with editing. Carrie Rodomar, librarian of University of Nicosia Medical school for assisting with methodology.
Footnotes
Shiloh Plaut- sole researcher and author of this manuscript including conception, organization, literature review, integration of information, findings analysis, manuscript preparation and writing.
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.
- 18.↵
- 19.↵
- 20.↵
- 21.
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.
- 56.
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.
- 66.
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.
- 78.↵
- 79.↵
- 80.↵
- 81.↵
- 82.↵
- 83.↵
- 84.↵
- 85.
- 86.↵
- 87.↵
- 88.↵
- 89.
- 90.
- 91.↵
- 92.↵
- 93.↵
- 94.↵
- 95.↵
- 96.
- 97.↵
- 98.↵
- 99.
- 100.
- 101.↵
- 102.↵
- 103.↵
- 104.
- 105.↵
- 106.↵
- 107.↵
- 108.↵
- 109.↵
- 110.↵
- 111.↵
- 112.↵
- 113.↵
- 114.↵
- 115.↵
- 116.↵
- 117.↵
- 118.↵
- 119.↵
- 120.↵
- 121.↵
- 122.↵
- 123.↵
- 124.↵
- 125.
- 126.
- 127.↵
- 128.↵
- 129.↵
- 130.
- 131.
- 132.
- 133.
- 134.
- 135.
- 136.
- 137.
- 138.↵
- 139.
- 140.
- 141.↵
- 142.↵
- 143.↵
- 144.↵
- 145.↵
- 146.↵
- 147.↵
- 148.↵
- 149.↵
- 150.↵
- 151.↵
- 152.
- 153.↵
- 154.↵
- 155.↵
- 156.↵
- 157.↵
- 158.↵
- 159.↵
- 160.↵
- 161.↵
- 162.↵
- 163.↵
- 164.↵
- 165.↵
- 166.↵
- 167.
- 168.↵
- 169.↵
- 170.↵
- 171.↵
- 172.↵
- 173.↵
- 174.↵
- 175.↵
- 176.↵
- 177.↵
- 178.↵
- 179.↵
- 180.↵
- 181.↵
- 182.↵
- 183.↵
- 184.↵
- 185.↵
- 186.↵
- 187.↵
- 188.
- 189.
- 190.
- 191.
- 192.
- 193.↵
- 194.↵
- 195.↵
- 196.↵
- 197.↵
- 198.↵
- 199.↵
- 200.↵
- 201.↵
- 202.↵
- 203.↵
- 204.↵
- 205.
- 206.
- 207.↵
- 208.↵
- 209.↵
- 210.↵
- 211.
- 212.
- 213.
- 214.↵
- 215.↵
- 216.↵
- 217.
- 218.
- 219.
- 220.↵
- 221.↵
- 222.↵
- 223.↵
- 224.
- 225.↵
- 226.↵
- 227.↵
- 228.↵
- 229.↵
- 230.↵
- 231.↵
- 232.↵
- 233.
- 234.
- 235.
- 236.↵
- 237.↵
- 238.↵
- 239.↵
- 240.↵
- 241.↵
- 242.↵
- 243.↵
- 244.↵
- 245.↵
- 246.
- 247.
- 248.
- 249.↵
- 250.↵
- 251.↵
- 252.↵
- 253.
- 254.
- 255.
- 256.
- 257.
- 258.↵
- 259.↵
- 260.↵
- 261.
- 262.
- 263.↵
- 264.↵
- 265.↵
- 266.
- 267.↵
- 268.↵
- 269.↵
- 270.
- 271.
- 272.↵
- 273.↵
- 274.
- 275.
- 276.↵
- 277.↵
- 278.↵
- 279.↵
- 280.↵




