
Abstract
Background The inherent complexities of condition such as tinnitus with cause and mechanism not known, presents lack of high-level evidence to make an inference on the treatment approaches. A comprehensive review cannot be performed owing to insufficient number of trials. Hence a scoping review approach was adopted to provide a broad overview on approaches for tinnitus management.
Objective To review the current evidence on prevalent treatment strategies used for tinnitus management and determine barriers and facilitators for adoption of treatment approaches in developed and developing countries.
Methods The present scoping review was performed in compliance with PRISMA ScR checklist. Literature search was carried out in PubMed, Scopus, google scholar and Cochrane database. Articles published between 2010-2021 mentioning therapeutic treatment strategies were included. However, therapies concentrating on symptomatic management were excluded. Evidence with highest scientific hierarchy such as systematic reviews (SRs) and randomized-controlled trials (RCTs) were considered. The context for the ScR was study-region based and included studies from high-income and low and middle-income countries (HICs, LMICs)
Results A total of 20 records were included with 11 SRs and 9 RCTs. Non-pharmacological interventions demonstrated moderate efficacy, including transcranial magnetic-(TMS) and direct current stimulation (tDCS), hearing aids (combined with sound generator or alone). No specific drug found to have mode of action pertaining to target root cause due to lack of clinical knowledge. Most of the trials used the same tools for tinnitus severity.
Conclusion Although several scoping reviews are published with exclusive focus on individual therapies, authors recommend umbrella review of systematic reviews to generate evidence-based practice consensus for tinnitus.
Introduction
Clinical care pathway is a major deterministic factor for better patient outcomes. Conventionally, it is decided based on clinical acumen. However, with the increasing clinical inclination towards evidence-based medicine, best available evidence and patient values and preferences have been also strongly recommended to consider while determining treatment course. Nevertheless, there are a few clinical conditions with a blurry picture in terms of standard clinical care, including Tinnitus. Tinnitus is a clinical condition in which patients hear a ringing sound in their ears, impacting their quality of life. It may be referred as “phantom auditory perception”1 with variety of sounds including – hissing, buzzing, clicking, chirping, ringing, whistling, or cricket-like sound, which can be intermittent or continuous.
Tinnitus is not a disease but might be a composite manifestation of various otological, neurological and cardiovascular disorders2, affecting an estimated 10-15% of adult population3. Epidemiologic data shows prevalence as 15% in USA4, 14.2% in Europe5, and similar in UK6, Asia7 and Africa8. It can be broadly classified as subjective and objective tinnitus. Subjective tinnitus, a more common type, refers to the perception of sound in absence of source or acoustic environment and can be perceived only by the patient. The rare type, objective tinnitus, refers to the sound produced by body and can be heard by the examiner too during the otologic examination. Other types include pulsatile, primary (idiopathic), secondary (underlying cause), acute (<6 months) or chronic (>6 months).
The condition can be distressing and debilitating and may have a negative impact on quality of life9. It may interfere with routine activities and can be bothersome. Individuals may experience anxiety, depression, irritability, sleep cycle disturbances, poor concentration, pain, and even suicidal thoughts in extreme cases. Along with personal and social impact, the economic impact is huge. Global cost analysis estimated the cost to health sector range from $67-107 billion, with 63-73% of global cost incurred to low- and middle-income countries (LMIC)10. The economic burden in UK is estimated to be £750 million per year11.
Even-though the exact cause and mechanism for the condition is not known, it may be associated with age-related hearing loss, middle ear infection, trauma, head injury, loud work environment, anxiety, depression, or ototoxic drugs like NSAIDs (non-steroidal anti-inflammatory drugs), antibiotics, chemotherapeutic agents12–14. The lack of proper mechanism makes it difficult to manage or treat the condition.
Despite several systematic reviews published on efficacy of several clinical interventions to cure the tinnitus, there is no food and drugs administration (FDA)approved, gold standard treatment or drug for tinnitus till date15. Several treatment pathways are identified through anecdotal evidence including but not limited to cognitive-behavioral therapy (CBT), tinnitus retraining therapy (TRT), biofeedback, psychoeducation or counselling, hearing aids, electrical stimulation, antidepressants, anticonvulsants, dietary supplements2,13,16–18. While its implications in practice can be over debate, due to lack of high-level of evidence. In addition, combination therapies have shown promising potential not only in terms of relief from tinnitus-like distressing condition but also improvement in the holistic health of the patient19–21.
Given such inconclusive inferences from the published systematic reviews (SRs) on efficacy/effectiveness of various clinical interventions, it is difficult to build the practice consensus despite of being highest on the evidence pyramid. Instead, a novel research concept has gained immense interest especially from policy perspective, known as “scoping review (ScR). It is a typical variant of the traditional systematic review, where rigorous specific attention towards any single interventions’ efficacy and safety is replaced by collation of evidence in a comprehensive and informative manner. Although there are several scoping reviews published on Tinnitus in the past, to the best of authors’ knowledge, no research provided holistic overview of the treatment options likely to be recommended in the actual treatment of tinnitus except only one. Makar S et al. in 2017 described an overview of therapies for the tinnitus; however, no information about its protocol registration was found. Also, mapping of reported content in the same ScR with PRISMA-ScR checklist was not possible due to the later release of revised checklist in 202022.
The objective of present scoping review is to provide an update to the previously published scoping review(s) on Tinnitus therapies as a whole with the complementary information. It also discussed barriers and facilitators for the effective adoption of published treatment strategies in the health system of developed and developing countries.
Material and Methods
Protocol registration
The protocol was registered in the open science framework registry (OSF), registration DOI: 10.17605/OSF.IO/R8D39
Study selection criteria
Study Design and Search Filters
Although being a scoping review, full-text systematic reviews and randomized controlled trials in the English were included. The rationale behind such design restrictions was to consider only the evidence with highest scientific hierarchy. Therefore, we excluded review articles, case reports, case series, cross-sectional studies, and observational studies. Focusing on recency of the data, records published before 2010 were not considered.
Population
Our target population for this scoping review included patients with any type of tinnitus. No age or gender related restrictions were applied as per the protocol. The tinnitus was defined as the sound in ears with or without any identifiable clinical cause. It included both subjective and objective types, where the former refers to the tinnitus perceived only by the sufferer and the later refers to the perception of tinnitus by both the examiner and sufferer through an objective assessment of the condition.
Concept
We included the records containing information about the efficacy and safety endpoints of pharmacological, phytomedicinal or non-pharmacological interventions for the treatment of tinnitus. Studies including details about secondary outcomes like effect on tinnitus-induced distress, anxiety or depression were also included. ScRs23–29 with focus on single intervention or on habituation-oriented therapy (Tinnitus Retraining Therapy, Cognitive Behavioral Therapies, etc.) were excluded to assess direct effect of the intervention unlike surrogate effect in terms of habituation with the noise resulting from tinnitus or masking of the same. In other words, studies assessing only effect of the intervention on improvement of quality of life from symptomatic relief or habituation were excluded.
Context
We included studies from high-income countries and low and middle-income countries.
Search Strategy
Preliminary search was performed on PubMed to identify the relevant search terms used in publications related to tinnitus. Following this step, a detailed search strategy was developed which included three databases – Cochrane, PubMed, Scopus, and Google Scholar. Cochrane search was performed using the string - “Tinnitus AND therap*” on the Cochrane website. PubMed based search was performed using AI-powered tool named VOODY (Genpro Research Inc.). The search strategy used for PubMed Search is as follows:
tinnitus[mh] OR tinnitus[tw] OR subjective tinnitus[tw] OR objective tinnitus[tw] OR pulsatile tinnitus[tw] OR primary tinnitus[tw] OR secondary tinnitus[tw] OR acute tinnitus[tw] OR chronic tinnitus[tw] OR chronic idiopathic tinnitus[tw] OR induced tinnitus[tw] OR drug induced tinnitus[tw] OR surgery induced tinnitus[tw] OR trauma induced tinnitus[tw] OR ringing buzzing*[tw] OR hearing loss[tw]
AND
management[mh] OR therapeutics[mh] OR surg*[tw] OR surgical management[tw] OR non-surgical management[tw] OR pharmacolog*[tw] OR prevention and control [tw] OR treatment [tw] OR therap*[tw] OR drug therap*[tw] OR radiological therap*[tw] OR psycholog*[tw] OR psychotherap*[tw] OR sound therap*[tw] OR cognitive behavioral therap*[tw] OR tinnitus retraining [tw] OR retraining therap*[tw] OR cochlear implant*[tw] OR acoustic therap*[tw] OR cervical spine therap*[tw] OR orthodontic therap*[tw] OR auditory stimul*[tw] OR transcranial magnetic stimul*[tw] OR passive music therap*[tw] OR active music therap*[tw] OR physical therap*[tw] OR exercise therap*[tw] OR myofunctional therap*[tw] OR acupuncture[tw] OR mindfulness based intervention*[tw] OR masking therap*[tw] OR tinnitus masking [tw] OR hearing aid*[tw] OR counsel*[tw] OR quality of life [mh] OR health related quality of life [mh] OR QOL [tw] OR HRQOL[tw] OR health care[tw] OR quality of health care[tw] OR standard of care [tw] OR patient satisfaction [tw] OR disability adjusted life year* [tw] OR quality adjusted life year*[tw] OR DALY*[tw] OR QALY*[tw]
AND
epidemiology[mh] OR economic[mh] OR economic*[tw] developed countr*[tw] OR developing countr*[tw] OR high income countr*[tw] OR middle income countr*[tw] OR upper middle income countr*[tw] OR low middle income countr*[tw] OR India[tw] OR UK [tw] OR USA[tw] OR Europe[tw] OR Canada[tw]
Additionally, targeted search was performed from additional sources like Google, American Tinnitus Association, British Tinnitus Association, All Indian Institute of Speech and Hearing (AIISH). Also, an exclusive targeted search for tinnitus related scoping review was done using PubMed database to identify the published similar scoping reviews.
The whole study selection was performed by two independent reviewers. Any discrepancy regarding inclusion was resolved by mutual agreement or consenting third reviewer.
Data charting
The data charting instrument/template was prepared and piloted using three articles. Necessary fields and sub-sections based on research question framework (PCC) were added before commencing the extraction process. Two independent reviewers performed the charting. The extraction items included: author, year of publication, study type, type of tinnitus, population demographic details, concept (intervention used, outcome measures), context (study region). Outcome measures was sub-divided into primary (tinnitus severity, loudness, depression, anxiety) and secondary (QoL, HRQoL, depression, anxiety) outcomes. The extracted data was reviewed for its accuracy by second reviewer. Any disagreement was resolved by mutual discussion or consensus from third reviewer. The charted data was presented using tabulation method.
Results
Study selection
An exhaustive literature search retrieved 4148 records from the following databases: PubMed (n =838), Scopus (n = 2441), Cochrane (n = 538), Google Scholar (n = 331). 754 records were removed during deduplication. Out of 3394 records screened, 3124 records were excluded based on non-relevance. Finally, 86 full text records were screened, out of which 20 records were included for qualitative synthesis. Adaptation was made in the original template of PRISMA-ScR flow diagram30 as we considered web content from websites of World Health Organization and American Tinnitus Association only as a supplementary data with no stringent eligibility criteria applicable. A detailed description of study selection process is shown in Fig.1 (PRISMA flow diagram).
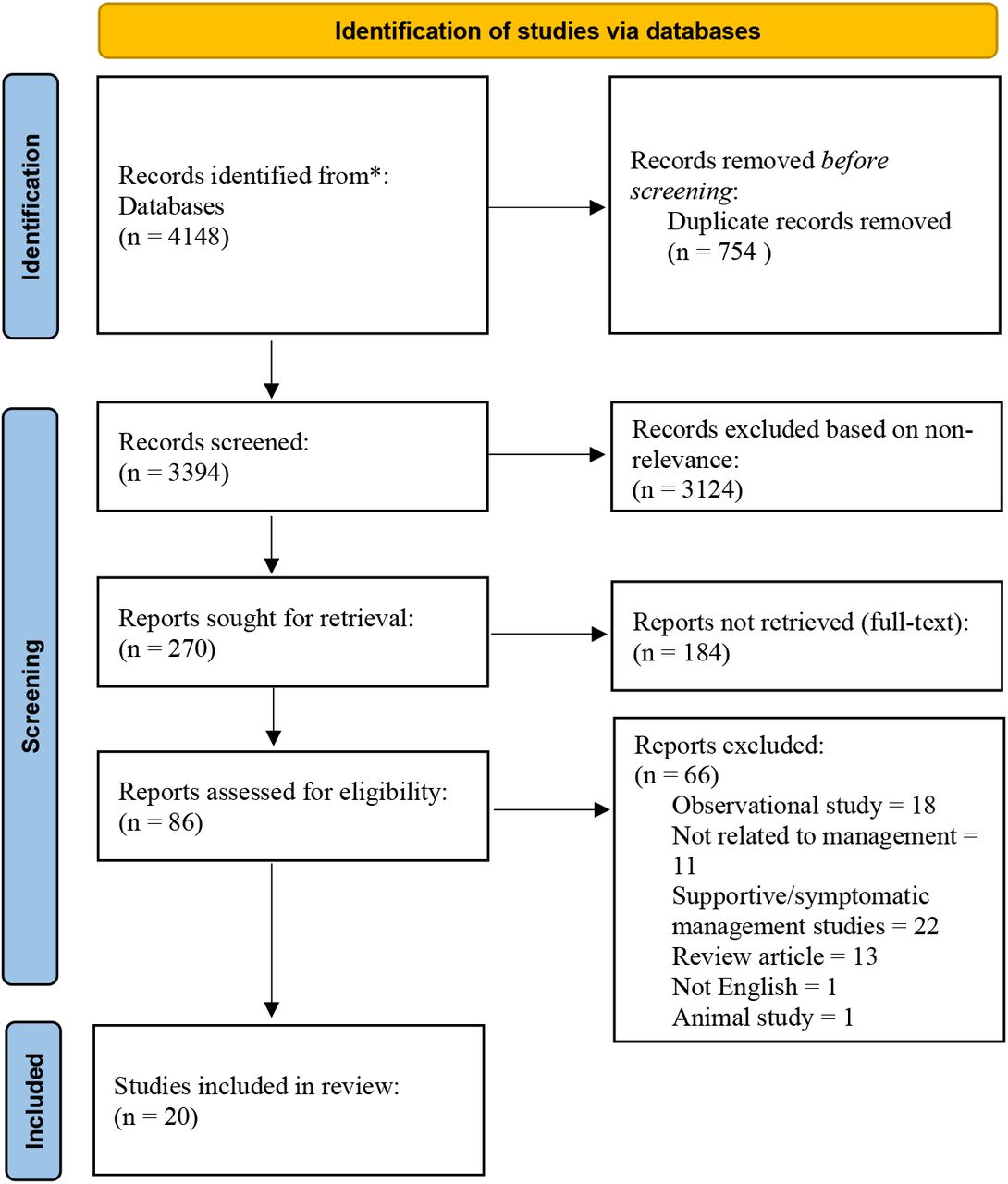
*PubMed (n = 838), Scopus (n = 2441), Cochrane (n = 538), Google Scholar (n = 331)
Report characteristics
Of the 20 included records, 11 were systematic reviews and 9 were RCTs. 6/9 RCTs were double-blinded, 5/6 RCTs intervening stimulation techniques were sham (inactive stimulation) controlled and 1 study was placebo-controlled (intervening drug AM-101). Study-region based findings suggested 2 records from United States of America (USA), 10 from Europe (Netherlands, United Kingdom (UK), Italy), 2 from Germany and Brazil, 1 from Middle east, and 1 multisite study (North America, Europe, Asia). Sample-size difference was present in the included studies, ranging from 20 participants to 343 participants with respect to RCTs, whereas systematic reviews included a highest of 1199 participants. Population in the included studies were >18 years age. Gender-based criteria was not mentioned in all included studies; however, 4 studies determined male:female ratio and found higher proportion of male (75.5%) compared to female (24.5%)31–34.
Study characteristics
Population
The review did not exclude records based on tinnitus type. Hence, various types of tinnitus were identified including chronic (n=559), acute (n=343), subjective (n=209), chronic-subjective (n=30), subjective-idiopathic (n= 590), chronic bilateral (n=21), acute inner-ear (n=248), chronic subjective unilateral/bilateral non-pulsatile primary tinnitus (n=53).
Concept
Tinnitus Severity Measurement Tools
Majority of the studies used Tinnitus Handicap Inventory (THI)32,34–41, Tinnitus Handicap Questionnaire (THQ)34,40,42,43. Other tools used for assessment of tinnitus outcome included Tinnitus Functional Index (TFI)31,36, Visual-Analog Scale (VAS)36,38,44, Beck Depression Inventory (BDI)34,40,41, Tinnitus Reaction Questionnaire (TRQ)34,40, Clinical Global Impression (CGI)38, Tinnitus Severity Index (TSI)41,45. One study each used Pittsburgh Sleep Quality Index (PSQI)41 to assess sleep disturbance and Hamilton Depression Rating Scale (HDRS)40 to assess depression. 22,24–31, THQ34,40,42,43. Other tools used for assessment of tinnitus outcome includes TFI31,36, VAS36,38,44, BDI34,40,41, TRQ34,40, CGI38, TSI41,45. One study each used PSQI41 to assess sleep disturbance and HDRS40 to assess depression.
Interventions
The interventions included three major categories: pharmacological (n = 2), complementary and alternative medicine (CAM) (n = 8) and non-pharmacological interventions (n = 10). Pharmacological and CAM interventions included AM-101 (NMDA receptor antagonist)33,46, zinc37, ginkgo biloba (GB) extract47, melatonin41, anti-depressant42, and anti-convulsant43. Whereas non-pharmacological interventions included transcranial magnetic stimulation (TMS)31,34,36,45, vagus nerve stimulation (VNS)32, transcranial direct stimulation (tDCS)38,44,48, devices such as hearing aid35,39 (alone or in combination with sound generator).
Outcomes
Outcomes were further sub-divided to primary and secondary outcomes. Table 1 presents the charted data for this project. Only 3 studies assessed secondary outcomes including depression, anxiety, and level of sleep disturbance.
Non-pharmacological interventions
Transcranial direct stimulation (tDCS)
3 studies (2 RCT, 1 SR) assessed chronic tinnitus using tDCS 38,44,48. The effects of tDCS were inclined towards anodal tDCS, whereas cathodal tDCS resulted in non-significant changes. Systematic review by Yuan et al.48 included studies performing single or repeated session of tDCS at current intensity of 1-2 mA. Similar outcome measured by Forogh et al.38, determined reduction (anodal tDCS); however, not significant. There was a moderate to significant reduction in tinnitus distress and loudness when applied to dorso-lateral prefrontal cortex (DLPFC) and auditory cortex (AC) region. The study also found reduction in tinnitus-related depression and anxiety specific to bifrontal cortex. Although, RCT by Garin et al.44 did not found such effect. Inference could not be constructed based on methodological issues including sample size and study period. Further, assessing safety outcomes, 36.4% patients had symptoms worsened as measured by one study38.28,34,38. The effects of tDCS were inclined towards anodal tDCS, whereas cathodal tDCS resulted in non-significant changes. Systematic review by Yuan et al.48 included studies performing single or repeated session of tDCS at current intensity of 1-2 mA. Similar outcome measured by Forogh et al.38, determined reduction (anodal tDCS); however, not significant. There was a moderate to significant reduction in tinnitus distress and loudness when applied to dorso-lateral prefrontal cortex (DLPFC) and auditory cortex (AC) region. The study also found reduction in tinnitus-related depression and anxiety specific to bifrontal cortex. Although, RCT by Garin et al.44 did not found such effect. However, inference could not be constructed based on methodological issues including sample size and study period. Further, assessing safety outcomes, 36.4% patients had symptoms worsened as measured by one study38.
Repetitive transcranial magnetic stimulation (rTMS)
4 studies intervened patients with chronic and subjective tinnitus using rTMS31,34,36,45. The studies used 1000-2300 pulses per session at frequency of 1 Hz. The studies found reduction in tinnitus severity31 and loudness45. Nevertheless, inference could not be made, subjected to difference in sample size and study follow-up period. Formanek et al.34 compared rTMS, sham stimulation and ginkgo biloba extract. THI score improved in all the groups; however, superiority cannot be obtained. With regard to safety outcome, temporal side-effects were observed in rTMS and sham stimulation group. Mennemeier et al.45 performed rTMS on tinnitus patients and correlated with PET scans. Although THQ and TSI shown improvement in tinnitus loudness, PET scans failed to reflect the same.
Vagus nerve stimulation (VNS)
Only one study32 intervened using VNS in patients with chronic sensorineural tinnitus, comparing VNS paired and unpaired with tones. 50% participant shown improvement in tinnitus severity after 42 days which increased to 56% after 84 days in VNS paired group.
Hearing-aids (HA)
HA were used in two studies and compared with combined (CD) device (HA and sound generator). The studies did not found difference in tinnitus severity and annoyance improvement among HA and CD as measured by THI.
Pharmacological interventions
Anti-depressants
Baldo et al.42 performed an SR on anti-depressant (nor-triptyline, a tricyclic anti-depressant) use in tinnitus. The findings suggest reduced tinnitus-specific depressive symptoms and improved QoL (trazodone, atypical anti-depressant). The findings were from single trials and pooled analysis described non-significant effect. Hence inference could not be made.
Anti-convulsants
A SR carried out by Hoekstra et al.43 assessed effect of anti-convulsants (lamotrigine, carbamazepine, flunarizine). The study determined improvement in tinnitus severity measured by THQ, THI, Tinnitus questionnaire (TQ) scales; however, not significant. The study also failed to show beneficial effect on HRQoL.33 assessed effect of anti-convulsants (lamotrigine, carbamazepine, flunarizine). The study determined improvement in tinnitus severity measured by THQ, TQ, THI, TEQ scales; however, not significant. The study also failed to show beneficial effect on HRQoL.
NMDA receptor antagonists
AM-101 is a NMDA(N-methyl-D-aspartate) receptor antagonist. A multi-site RCT described increase in hearing threshold in <7% patients33. Another study by Heyning et al.52 carried out dose-dependent study. There was a significant improvement in tinnitus loudness, sleep disturbance in high-dose (0.81mg/ml) group. However similar effect was not observed in minimum masking level (MML). Mild adverse effects were observed. The studies suggest repeated dose of AM-101 to be safe and well-tolerated.
Complementary and Alternative Medicine
Ginkgo Biloba Extract (GB)
The findings from SR performed to evaluate effects of GB extract in tinnitus patients was suggestive of reduced tinnitus severity, though the effect was observed to specific EGb 761 extract and no other extracts of GB47. No significant differences were found comparing rTMS, sham and GB extract34.
Zinc supplementation
Effects of oral zinc supplement was evaluated in patients with subjective tinnitus37. However, the study failed to conclude improvement in tinnitus symptoms due to lack of evidence. 2 out of 3 studies included in SR described mild adverse effects.
Melatonin
One study reviewed the effects of melatonin at dose of 3mg when used alone and in combination with sulpiride or sulodexide41. The review was unable to demonstrate effect on tinnitus severity; however, melatonin alone improved sleep disturbance.
Our study included two SRs assessing multidisciplinary treatment options40,49. The studies showed significant improvement and recommended cognitive-behavioural therapy (CBT) along with counselling. With regards to pharmacological intervention, only anti-depresssant showed potential for beneficial effect.
Discussion
Owing to inherent complexity of the clinical condition for the patients with tinnitus and failure to identify and correlate the root cause and associated mechanism, sufficient number of trials have not been possible to conduct in case of the tinnitus. To overcome these challenges, first step was proposed to enlist the possible interventions, scales used, and outcomes assessed for tinnitus to identify research lacunae if any. This was accomplished by the recommended evidence synthesis method - Scoping review. Being an update, this scoping review did not consider already published information but presented complementary information to provide a clear picture about all possible therapies while determining the holistic care pathway for the tinnitus. Also, broad spectrum of information covering both HICs and LMICs introduced comprehensiveness in data charting process. However, recency of the information was ensured through limiting studies between timeframe 2010-2021 (from last 10 years). This also helped to understand current vistas in the therapeutic management of the tinnitus as well as the directions for tinnitus research progress.
The review included only systematic reviews (11) and RCTs (9), contributing to highest level of evidence strength. 8 out of 20 studies included in this scoping review intervened using stimulation technique (TMS, tDCS, and VNS). Overall, the stimulation showed reduction in tinnitus severity and perception. Although, the effects were dependent of the region of application and the polarity (anodal/cathodal). Yuan et al.39 determined moderate to significant reduction in tinnitus loudness, distress and tinnitus-related depression and anxiety when tDCS was applied to DLPFC and auditory cortex AC region. The reason behind the inclination of findings towards DLPFC and AC might be the involvement of frontal region in pathophysiology of tinnitus42,43. Both rTMS and tDCS reduces the abnormal neuronal hyperactivity44,45 and modulates tinnitus transiently; however, long-term effects were not observed46. Moreover, tDCS demonstrated clinical and cost-effectiveness47.
HA amplification reduces tinnitus perception and help in coping, and masks the tinnitus using amplified sound. CD are relatively new approach and have shown to reduce tinnitus severity26,30. However, superiority was not established among HA and CD. Nevertheless, recent advancement pertaining to use of artificial intelligence techniques, acoustic sensors have been developed to analyze the surrounding environment, reduce noise, and adjust the sound based on hearing preferences. Consensus-based guidelines recommend use of HA for persistent and bothersome tinnitus, and often considered as first-line treatment48–50.
On the other side, there was questionable efficacy of pharmacological interventions to treat or cure tinnitus. Nevertheless, therapies oriented to achieve surrogate effect through addressing complex comorbidities aligned in patients with tinnitus such as depression, anxiety, insomnia was evident. For example, anti-depressants have potential for reduction in tinnitus-specific depression31,33,51. Novel approaches including AM-101 (NMDA receptor antagonist), anti-convulsant, zinc, ginkgo biloba and more, have shown to be effective in reducing tinnitus severity. Contradictory outcomes were determined from two trials which assessed efficacy of AM-10124,37. However, the studies indicate the intervention to be safe and well-tolerated for repeated doses. Besides, the study determined majority of RCTs (7/9) were performed in HICs, indicating need of the hour for comparative effectiveness research for the tinnitus care solutions using empirical treatments in case of LMICs.25,29.
A similar scoping review by Makar et al.21 described the interventions with surrogate effect on tinnitus, including counselling, tinnitus masking, tinnitus retraining therapy (TRT), cognitive behavioral therapy (CBT), relaxation, and attention diversion in tinnitus patients. Complementing to the same, our study described role of non-pharmacological as well as adjuvant pharmacological treatment modalities which may play little to moderate role in tinnitus management. Unlike previous scoping review(s) which either focused on interventions with surrogate effect or specific to individual interventions, we understand our study demonstrated uniqueness with enlisting the details of interventions with highest quality of supporting evidence. In addition, our scoping review data charting included every detail about study interventions, severity scales, outcomes, and recommendations. Thus, it helped better understand methodological quality of the included records. Albeit it is to be noted that scoping review does not emphasize on critical appraisal of collected evidence, it is useful to chart information in comprehensive manner to guide the further research. For example, although it was not primary aim to assess the effect on QoL or HR-QoL, we included the variables considered for assessing secondary objective i.e., effect of QoL in relation with the tinnitus. Other scoping reviews have been performed on individual therapies such as psychotherapy52, hearing aids53, amplification technique54, tDCS55. However, failed to make recommendation due to lack of quality evidence.20
Limitation
Despite a well-devised search strategy, the study could not demonstrate any actionable insights based on collected evidence. This could be partially attributable to limited access to subscription journals and study search restricted for only full-text free articles. Also, we were not able to demonstrate the charted data in an easily interpretable form due to time constraints. We did not obtain any substantial information from the web-portals of associations despite their mention as a potential source of information. Lastly, we acknowledge several significant changes to the registered protocol version on OSF platform, which were deemed mandatory to be implemented during the course of project execution. This included 1) Removal of objective to assess health systems related barriers and facilitators due to lack of relevant secondary data and its out-of-scope nature 2)The study team included 3 investigators ; however, additional research team members including ENT specialists and a family physician was introduced to the team to expedite the manuscript authoring work and for the quality improvement purposes and 3) Inconsistencies were found between the source of information mentioned in methods section and eligibility criteria in appendix. As the resolution, eligibility criteria were approved in its original form without any relaxation regarding the information source type (textual note, non-scientific record).
Futuristic Implications for Research and Practice
Continual advancements are taking place in the field, be it novel devices, implant system56 or surgery. Although there is no surgical treatment to cure tinnitus, neuromodulation of trigeminal nerve seems promising approach and requires further investigations in future57. Deep brain stimulation technique has been used for Parkinson, psychiatric conditions showing tinnitus relief as a beneficiary effect58. Clinical trials investigating DBS in tinnitus patients is recommended with intensification of current level of scientific rigor. Also, the curative potential of brain surface implants needs a serious attention of researchers working in the area of experimental therapies for tinnitus.
Given the inconclusive evidence with poor strength to advocate any specific treatment option or combination of a few, it is difficult to generate the practice consensus with high degree of generalizability. However, as a next step, along with ongoing research and development initiatives, umbrella review – review of systematic reviews - could be recommended with exclusive focus on the published systematic reviews. Moreover, the interventions with moderate effect must be studied in larger group of patients with robust RCT designs with minimal bias and validated questionnaires.
Conclusion
The present scoping review charted complementary evidence about the effect of various non-pharmacological and pharmacological interventions being used for tinnitus, which were different than those published in previous scoping review within Indian context. Moderate improvement has been shown for r-TMS and t-DCS, warranting large-scale research to further investigate region-specific and intensity level-specific dependency of the effect of respective interventions. The stimulation presented partial effect and long-term effect was not established. To summarize, complexity of tinnitus and inconclusive strength of the available research evidence demands intensification of translational research and encouragement of rigorous knowledge dissemination for the development of practice consensus on tinnitus in the near future.
Data Availability
All the data charted in the study is available in public domain and can be accessed using bibliography.
Conflicts of Interest
The authors for this paper have no conflicts of interest to declare.
Funding
This study received no funding from any agency in public, commercial or not-for-profit sectors.





{kind=link}