
Abstract
Several studies have revealed either self-reported chemosensory alterations in large groups or objective quantified chemosensory impairments in smaller populations of patients diagnosed with COVID-19. However, due to the great variability in published results regarding COVID-19-induced chemosensory impairments and their follow-up, prognosis for chemosensory functions in patients with such complaints remains unclear. Our objective is to describe the various chemosensory alterations associated with COVID-19 and their prevalence and evolution after infection. A cross-sectional study of 704 healthcare workers with a RT-PCR confirmed SARS-CoV-2 infection between 28/2/2020 and 14/6/2020 was conducted 3 to 7 months after onset of symptoms. Data were collected with an online questionnaire. Outcomes included differences in reported chemosensory self-assessment of olfactory, gustatory, and trigeminal functions across time points and Chemosensory Perception Test scores from an easy-to-use at-home self-administered chemosensory test. Among the 704 participants, 593 (84.2%) were women, the mean (SD) age was 42 (12) years, and the questionnaire was answered on average 4.8 (0.8) months after COVID-19. During COVID-19, a decrease in olfactory, gustatory, and trigeminal sensitivities were reported by 81.3%, 81.5% and 48.0% respectively. Three to seven months later, reduced sensitivity was still reported by 52.0%, 41.9% and 23.3% respectively. Chemosensory Perception Test scores indicate that 19.5% of participants had objective olfactory impairment. These data suggest a significant proportion of COVID-19 cases have persistent chemosensory impairments at 3 to 7 months after their infection but the majority of those who had completely lost their olfactory, gustatory, and trigeminal sensitivity have improved.
Introduction
Coronavirus disease-2019 (COVID-19) is an ongoing major public health challenge. Olfactory dysfunction (OD) is a specific symptom that may affect approximately 60% of patients suffering from COVID-191-3, and is now considered as a stronger indicator of COVID-19 than fever, cough and shortness of breath4.
Investigation of the long-term effects of COVID-19 on chemosensory function is hindered by the recent onset of the pandemic and other challenges: First, many studies include a relatively small number of participants5, 6 or participants with severe forms of COVID-197, 8. Secondly, many studies include participants with an unclear diagnosis of COVID-19, and/or self-diagnosis 9, 10. Lastly, while individuals with anosmia can usually evaluate their olfactory function with accuracy11, this self-assessment is often challenging for individuals with intermediate forms of OD (e.g., hyposmia)12.
OD can be quantitative or qualitative. Quantitative OD defines a reduction of olfactory sensitivity which can be either a complete (anosmia) or a partial (hyposmia) loss of olfactory function13. Qualitative OD describes an altered perception of olfactory stimuli, such as parosmia, the perception of qualitatively altered smells, or phantosmia, the perception of a smell in the absence of an objective odorant13, 14. Overall, the prevalence of OD in the general population is around 20% 15, 16, and all different forms of OD are associated with reduced quality of life and increased risk of depression and anxiety17. In addition to OD, COVID-19 also appears to affect other chemosensory functions, i.e. gustatory and trigeminal perception 9, 18.
To comprehensively understand long-term olfactory, gustatory, and trigeminal alterations after COVID-19, we analyzed questionnaire responses from a cohort of healthcare workers infected with SARS-CoV-2 during the first wave of the pandemic (February -June 2020). We also developed a Chemosensory Perception Test (CPT), a formal test employing common household odorants and tastants, to enable accessible yet accurate self-evaluation of chemosensory functions.
Materials and Methods
Participants
Participants were recruited from a Quebec healthcare worker cohort who have had SARS-CoV-2 infection between 28/2/2020 and 14/6/2020. They were part of a study from the Institut National de Santé Publique du Québec and had agreed to be contacted for other research projects19. Inclusion criteria were (1) RT-PCR confirmed COVID-19 (2) above 18 years of age, (3) French or English speakers, (4) completed the online questionnaire, and (5) did not report of other respiratory diseases (bacterial or viral infection, or/and allergies with rhinorrhea) within 2 weeks prior to questionnaire completion or chronic sinusitis (Figure 1).

Flowchart of the study design. INSPQ: Institut national de santé publique.
This study was reviewed and approved by the research ethics board of the CHU de Québec – Université Laval (MP-20-2021-5228) and all protocols were reviewed by an independent Scientific Review Committee. This study also complies with the Declaration of Helsinki for Medical Research Involving Human Subjects. All participants provided an online informed consent prior to participation. The study received funding from the Fonds de recherche du Québec-Santé. No compensation or incentive was offered for participation. Data were collected from August 11 to October 29, 2020. Up to four attempts were made to reach by email potential participants. At the time of data collection, participants were 3-7 months after the onset of COVID-19 symptoms.
Online questionnaire
All participants were asked to complete an online questionnaire which was adapted from the core questionnaire of the Global Consortium on Chemosensory Research9.
Demographic information
In the first part of the questionnaire, demographic information was collected from all participants. Participants were then instructed to provide medical history and indicate the presence of specific COVID-19 symptoms (Figure 2).

Left, Self-rating of olfaction and reporting of CPT using VAS through the web-based interface, as viewed by the participant. Right, Sections of the online questionnaire. VAS: visual analog scale.
Chemosensory self-assessment
Participants were asked to self-evaluate and report their olfactory, gustatory, and trigeminal sensitivity using a 10-point visual analog scale (VAS; Figure 2) for three timepoints: (1) before SARS-CoV-2 infection, (2) during SARS-CoV-2 infection and (3) at questionnaire completion. Further, information on the presence of parosmia or phantosmia following the infection20 and alterations in the 5 tastes (sweet, salty, sour, bitter, umami) was collected.
Chemosensory Perception Test (CPT)
Items commonly found in North American households were used to assess participants’ olfactory and gustatory functions, as odor intensity is the best single predictor to classify individuals with normosmia21. Participants had to smell three substances (peanut butter, jam/jelly, and coffee) and rate odor intensity on a 10-point VAS (0: no smell at all; 10: very strong smell). We obtained olfactory scores by averaging these ratings. Pilot data on a total of 93 participants show these scores to accurately detect OD when compared to the Sniffin’ Sticks (cut-off score: 6/10; sensitivity: 0.765; specificity: 0.895; Supplement 3). Participants were asked to prepare saline and sweet water by dissolving respectively a teaspoon of salt or 3 teaspoons of sugar in a cup (250 mL) of lukewarm water. Then, they were asked to taste saline and sweet water and to rate taste intensities on a 10-point VAS. We obtained gustatory scores by averaging these ratings.
Statistical Analyses
A Python script (Python 3.7.5, Python Software Foundation, https://www.python.org) was used to process raw questionnaire data and to calculate the number of participants reporting COVID-19 symptoms, chronic conditions and recent respiratory illnesses. Processed data were analyzed and visualized with SPSS 26.0 (Armonk, NY: IBM Corp), GraphPad Prism 8.3.1 (GraphPad Prism Software, San Diego, CA) and Raincloud plots22.
Parametric (ANOVA) or non-parametric (Friedman) tests were chosen depending on whether normality assumption was fulfilled. To evaluate the effects of COVID-19 on modality (olfactory, gustatory, and trigeminal) and time (prior to, during and after COVID-19 infection), for gender (women, men), repeated measures (rm) ANOVA with age as a covariate were computed. To disentangle interactions, separate rmANOVA were carried out for individual modalities and timepoints with the same factors. Greenhouse-Geisser corrections were used for sphericity and Tukey’s multiple comparisons test were used for post-hoc comparisons. Friedman’s test was followed by Dunn’s post-hoc test to correct for multiple comparisons. To assess the correlation between self-reported olfactory, gustatory, and trigeminal abilities and results of the CPT, Pearson correlation coefficient or Spearman’s rank correlation coefficient was used. For all statistical tests, alpha was set at 0.05. All results are expressed as mean (SD) unless otherwise specified.
Results
Characteristics of participants
A total of 704 healthcare workers (593 (84.2%) women, mean age of 42.0 (SD:11.7, range 18 – 70) years were included. The questionnaire was completed on average 4.8 (SD: 0.8, range 3-7) months after symptoms onset. COVID-19 symptoms reported by the 704 participants are listed in Table 1.
COVID-19 symptoms of the 704 participants.
Quantitative disorders
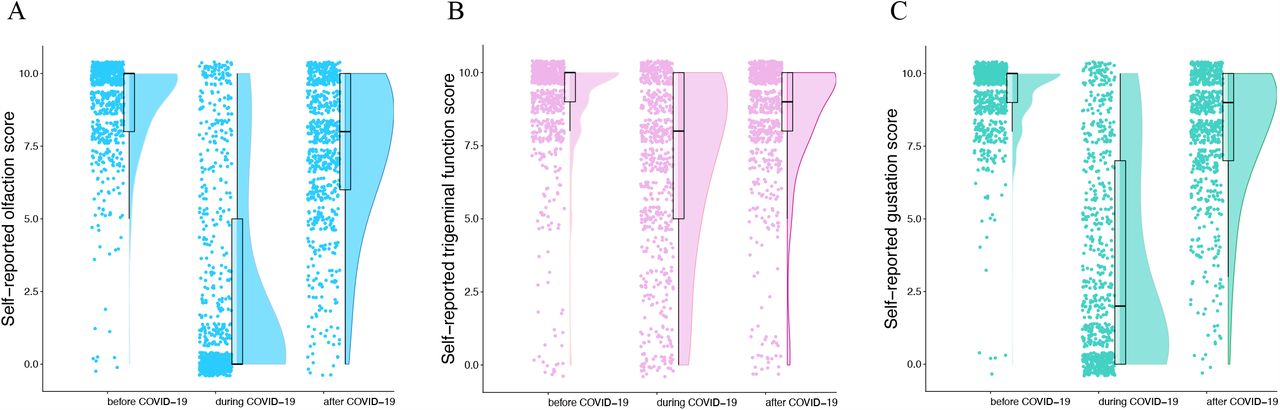
Before COVID-19, average self-reported score was 9.0 (1.6), 9.2 (1.3) and 8.9 (1.9) of 10 for olfaction, gustation and trigeminal function, respectively. Among participants, 0.9%, 0.7% and 1.8% respectively reported an absence of olfaction, gustation and trigeminal function (score 0; Figure 3). During COVID-19, average self-reported score was 2.6 (3.6) for olfaction, 3.4 (3.6) for gustation, and 7.0 (3.0) for trigeminal sensitivity. In the 704 participants, 51.1%, 33.5% and 5.7% reported absence of olfaction, gustation and trigeminal function. At time of questionnaire completion, mean scores were 7.4 (2.5), 8.0 (2.2) and 8.5 (2.2) for olfaction, gustation and trigeminal function respectively and absence of chemical senses was reported respectively by 1.4%, 0.7% and 2.3%.

Raincloud plot representing self-reported scores for olfaction, gustation, and trigeminal function before, during and after COVID-19. Ratings from individual participants are displayed as dots. Boxplots show the first to third quartiles, horizontal line denotes the median, and whiskers denote 1.5 times interquartile range. Compared to baseline, self-reported scores of olfaction, gustation and trigeminal function were significantly lower during COVID-19 and have not fully returned to baseline values 5 months after COVID-19.
Compared to the baseline chemosensory functions before COVID-19, 572 (81.3%), 574 (81.5) and 338 (48.0%) reported lower olfactory, gustatory, and trigeminal sensitivity during COVID-19. Olfactory and gustatory dysfunction were present in similar proportions (χ2(2, N=704) =0.02, P=.891) and were different to trigeminal (olfaction: χ2(2, N=704) = 174.81 P<.001; gustation: χ2(2, N=704) = 174.56 P<.001). Three to seven months after the infection, 366 (52.0%), 295 (41.9%), 164 (23.3%) reported lower olfactory, gustatory, and trigeminal sensitivity compared to before COVID-19 (Table 2). These proportions were significantly different between all three chemosensory systems (χ2(2, N=704) = 123.46, P<.001).
Self-reported chemosensory alterations by age group and gender during and 3 to 7 months following COVID-19 (n=704).
Overall, there were significant effects of modality (F(2,1402)=42.83,P<.001, ; olfactory<gustatory<trigeminal; all P<.001), time (F(2,1402)=118.47, P<.001,
; olfactory<gustatory<trigeminal; all P<.001), time (F(2,1402)=118.47, P<.001,  ; during<after<before; all P<.001), and gender (F(1,701)=5.52, P=0.019,
; during<after<before; all P<.001), and gender (F(1,701)=5.52, P=0.019,  ; women<men) and significant interactions between these factors (modality*time, modality*time*gender; all P<.001) on chemosensory self-evaluation. To disentangle these interactions, we analyzed data separately per chemosensory modality and time points.
; women<men) and significant interactions between these factors (modality*time, modality*time*gender; all P<.001) on chemosensory self-evaluation. To disentangle these interactions, we analyzed data separately per chemosensory modality and time points.
Chemosensory modality
With regards to olfactory function, significant main effects of time (F(2,1402)=165.07, P<.001  ; during<after<before; all P<.001; Figure 3A), age (F(1,701)=4.42, P=.012,
; during<after<before; all P<.001; Figure 3A), age (F(1,701)=4.42, P=.012,  ) and gender (F(1,701)=4.42, P=.036,
) and gender (F(1,701)=4.42, P=.036,  ; women < men) were revealed. In addition, we observed significant interactions of time*age (F(2,1402)=23.39, P<.001,
; women < men) were revealed. In addition, we observed significant interactions of time*age (F(2,1402)=23.39, P<.001,  ) and time*gender (F(2, 1402)=21.69, P<0.001,
) and time*gender (F(2, 1402)=21.69, P<0.001,  ).
).
With regards to gustatory function, we observed significant main effects of time (F(2,1402)=102.97, P<.001,  ; during<after<before; all P<.001; Figure 3B) and gender (F(1, 701)=9.80, P=.002,
; during<after<before; all P<.001; Figure 3B) and gender (F(1, 701)=9.80, P=.002,  ; women<men), but no effect of age. We also observed significant interactions of time*age (F(2, 1402))=5.97, P=.005,
; women<men), but no effect of age. We also observed significant interactions of time*age (F(2, 1402))=5.97, P=.005,  ) and time*gender (F(2, 1402))=20.02, P<.001,
) and time*gender (F(2, 1402))=20.02, P<.001,  ).
).
With regards to trigeminal function, we observed significant main effects of time (F(2,1402)=3.91, P=.020,  ; during<after<before; all P<.001; Figure 3C), and age ((1,701)=5.08, P=.025,
; during<after<before; all P<.001; Figure 3C), and age ((1,701)=5.08, P=.025,  ) but no effect of gender. We also identified significant interactions of time*age (F(2, 1402)=4.70, P=.016,
) but no effect of gender. We also identified significant interactions of time*age (F(2, 1402)=4.70, P=.016,  ) and time*gender (F(2, 1402)=4.50, P=.019,
) and time*gender (F(2, 1402)=4.50, P=.019,  ).
).
Time point
With regards to chemosensory function before infection, we observed a significant effect of gender (F(1,701)=8.52, P=.004,  ; men < women), but not of modality, age nor interactions. During COVID-19, we observed a significant effects of modality (F(2, 1402)=96.714, P<.001,
; men < women), but not of modality, age nor interactions. During COVID-19, we observed a significant effects of modality (F(2, 1402)=96.714, P<.001,  ; olfaction<gustation<trigeminal; all P<.001), gender (F(1, 701)=21.98, P<.001,
; olfaction<gustation<trigeminal; all P<.001), gender (F(1, 701)=21.98, P<.001,  ; women<men), and age (F(1, 701)=4.74, P=.030,
; women<men), and age (F(1, 701)=4.74, P=.030,  ). Further, we found significant interactions modality*age (F(2, 1402)=24.185, P<.001,
). Further, we found significant interactions modality*age (F(2, 1402)=24.185, P<.001,  ) and modality*gender (F(2, 1402)=6.76, P=.002,
) and modality*gender (F(2, 1402)=6.76, P=.002,  ). Finally, after infection, we observed a significant effect of modality (F(2, 1402)=9.91, P<.001,
). Finally, after infection, we observed a significant effect of modality (F(2, 1402)=9.91, P<.001,  ; olfaction<gustation<trigeminal; all P<.015), but not of gender or age, nor any interaction.
; olfaction<gustation<trigeminal; all P<.015), but not of gender or age, nor any interaction.
Compared to baseline (before infection), changes in chemosensory function were correlated for all modalities during infection (olfaction-gustation: ρ=0.69; gustation-trigeminal: ρ=0.43; olfaction-trigeminal: ρ=0.33; all P<.001, Figure 4 A-C) and after infection (olfaction-gustation: ρ=0.69; gustation-trigeminal: ρ=0.40; olfaction-trigeminal: ρ=0.36; all P<.001, Figure 4 D-F).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Red squares, correlations between alterations in olfaction, gustation, and trigeminal functions during COVID-19. Grey hexagons, correlations between alterations in olfaction, gustation, and trigeminal functions after COVID-19. Darker colors indicate higher occurrence.
Qualitative disorders
Among included participants, 78 (11.1%) reported parosmia, 73 (10.4%) experienced phantosmia and/or 82 (11.6%) had waxing and waning of olfaction following infection. In addition, 42 (6.0%) claimed that they experienced other forms of OD (hyposmia to specific substances, hyperosmia, parosmia only at high concentrations or slow identification times). Furthermore, 335 (47.6%) participants reported changes to perception of sweet, 338 (48.0%) salty, 293 (41.6%) sour, 309 (43.9%) bitter and 281 (39.9%) umami. A total of 275 (39.1%) participants reported alterations in all 5 tastes.
Chemosensory Perception Test
Among the 704 participants, 137 (19.5%) had a CPT score suggestive of OD. Mean CPT scores were lower for olfaction than gustation (7.84 (1.78) vs 8.42 (2.31); Z=8.193, P<.001). Neither age nor gender had an effect on CPT scores. CPT scores correlated with self-reported chemosensory abilities at testing time (olfaction: ρ=0.67; gustation: ρ=0.51; P<.001 for both).
Discussion
This study reports chemosensory dysfunction 3 to 7 months following SARS-CoV-2 infection in a large cohort of RT-PCR-confirmed healthcare workers. In addition to confirming the now well-established detrimental effect of acute COVID-19 on all three chemosensory systems (olfactory, gustatory, trigeminal), our major findings are: (1) the detrimental effect of COVID-19 lasts beyond the acute phase after the infection, half of those affected indicated that olfactory function had not returned to the baseline levels 3 to 7 months later, while 20% of infected participants reported scores in a formal test that are consistent with the presentation of hyposmia/anosmia; (2) approximately 10% of the patients exhibit parosmia and/or phantosmia; (3) women are more heavily affected than men.
We observed chemosensory dysfunction in the acute phase of COVID-19, which was most pronounced for olfactory function, but less so for gustatory function and even less for trigeminal function. The proportion of participants describing OD and GD in the acute phase of COVID-19 in this study was comparable to earlier studies23. Nevertheless, on average 4.8 months after infection and thus well after the acute phase, approximately 50% and 40% of patients reported persistent alterations in olfactory and gustatory sensitivity, respectively; these numbers are higher than what has been reported24, 25.
We found a moderate-to-strong correlation between self-reported olfactory and gustatory changes, which were stronger than with self-reported trigeminal changes. This could be due to similar pathophysiological alterations in the olfactory and gustatory systems and their differences from that of the trigeminal system. Knowing that the general population often mixes up retro-olfaction (perceiving odors from the substances in the mouth traveling posteriorly and rostrally to the olfactory epithelium) with taste, an alternative explanation would be a misunderstanding of this nuance by participants despite the fact that specific definitions for each modality were given26,27. The latter hypothesis is more probable since the correlation between gustatory self-report and CPT gustatory scores using strict gustatory stimuli (salt, sugar) is lower than the correlation between olfactory self-report and CPT olfactory scores.
Moreover, approximately 10% reported parosmia and/or phantosmia following SARS-CoV-2 infection. These qualitative smell disorders usually involve unpleasant olfactory sensations (rotten eggs, sewage, smoke). While the exact patho-mechanism of parosmia and phantosmia are still to be elucidated, parosmia is probably linked to altered peripheral input/central processing of olfactory stimuli28. Importantly, patients with postviral OD and parosmia exhibit better recovery rates following olfactory training than those without parosmia29. Follow-ups will determine to what extent parosmia predicts a better outcome.
Women’s chemical senses were more affected than men by the infection. Women typically have better scores in olfactory testing than men 30. In turn, women exhibit a higher prevalence and a longer persistence of postviral OD31, 32, in line with our results. Gender differences could be explained by a multitude of neuroendocrine, social, and cognitive factors31. This suggests that the burden of COVID-19-related OD is more important for women than for men.
Different theories have been proposed to explain the persistence of OD in certain individuals, ranging from olfactory epithelium dysfunction to central nervous system infection 33-35. Since cells of the olfactory epithelium possess the ability to regenerate, the re-establishment of olfactory function is possible in the context of postinfectious OD 36, as well as in COVID-19-related OD, where 75-85% of the affected individuals recovered olfactory function within 60 days 24, 37. In addition to OD and GD, TD has also been reported in patients with COVID-19 9, 18. Our study indicates chemosensory dysfunction in 18.9% of participants as measured by the CPT 3 to 7 months after infection.
Persistent chemosensory dysfunctions may be a sign of chronic central nervous system alterations38, 39, and there is now evidence that SARS-CoV-2 can infect olfactory sensory neurons in humans40. Other viruses, such as the Japanese encephalitis virus, Varicella-Zoster virus, measles virus, human immunodeficiency virus and CoVs, were shown to invade the CNS41. Febrile seizures, loss of consciousness, convulsions, ataxia, status epilepticus, encephalitis, myelitis, neuritis and extrapyramidal symptoms are among extra-pulmonary symptoms that have been described42. The persistence of postinfectious neurological symptoms may contribute to the development or aggravation of chronic neurological diseases such as Parkinson, multiple sclerosis, or psychiatric outcomes41, 43-51. These patients should be followed up to document the development of neurological sequalae.
Olfactory and other chemosensory dysfunctions may have detrimental effects. First, affected individuals can expose themselves to harmful substances such as smoke, gas or spoiled food52, 53. It may trigger dysfunctional nutritional patterns like increased salt and sugar consumption and anorexia54, 55. Individuals with OD also have higher rates of anxiety and depression17, 56. Moreover, a functioning olfactory system may be a necessity in some workplaces such as in healthcare, where staff are required to have the ability to detect and qualify the smell of urine, excrement, infected wounds or abnormal smells of breath57. Currently, there is no approved therapy for COVID-19-induced OD, although olfactory training has a significant effect on olfactory function according to studies on other viral infections58-60. Most importantly, long-term follow-up of these patients will be necessary to assess other signs of neurological damage.
Limitations
Given the cross-sectional design of the study, a recall bias is possible for all self-reported peri-SARS-CoV-2 infection values before or during the SARS-CoV-2 infection due to the 3-to-7-month gap. This study did not control for potential confounding factors like race and level of education. Finally, the CPT requires further validation for its gustatory and trigeminal components, and it relies on substances found in participants’ homes, which may lead to variation in test results due to the differences in the brand, quality, or expiration date of substances and consequently, their ability to trigger equal sensorineural responses.
Conclusions
Nearly two thirds of SARS-CoV-2 infected patients had chemosensory impairments during their infection and despite improvements, impairments persist in more than half of them 3 to 7 months after COVID-19. Quantitative and qualitative olfactory dysfunction as well as persisting gustatory and trigeminal deficits were common in the cohort presented in this study. Given the frequency of these problems and the possible neurological underpinnings of these observations, it will be critical to understand the underlying mechanisms of these chemosensory dysfunctions, their evolution, and possible therapeutic options.
Data Availability
Data can be made available upon request.
Supplementary 1
Validation of the Chemosensory Perception Test
This study was reviewed and approved by the research ethics board of the Université du Quebec à Trois-Rivières (CER-20-268-08-01.04). All participants provided a verbal or written informed consent prior to participation.
Experiment 1
Methods
Participants were recruited among previously tested groups. Olfactory testing was performed using the standardized Sniffin’ Sticks test at our laboratory from 2016 to 2019. Exclusion criteria was any perceived changes of their sense of smell since previous testing. Participants were distributed into 2 groups based on their Threshold-Discrimination-Identification (TDI) scores. The first group consists of participants with normal olfactory function (normosmia), defined as TDI scores above 30.561. The second group had subjective olfactory dysfunction and equivalent TDI scores. Participants were administered CPT by means of a telephone interview.
Results
TDI scores in the first group range from 32.5 to 41.5 (N= 19, 9 women and 10 men, age range [60-78]). TDI scores in the second group ranged from 8 to 30.25 (N= 17, 7 women and 10 men, age range [57-77]). CPT scores were positively correlated with the Sniffin’ Sticks (ρ=0.837, P<0.001). A cut-off score of 6 at the CPT had a sensitivity of 0.765 and specificity of 0.895.
Experiment 2
Methods
Participants were recruited among previously tested groups, participants from this cross-sectional study and in the public via social media. They were administered the University of Pennsylvania Smell Identification Test (UPSIT) (which was sent by mail) and the CPT under direct supervision through videoconferencing. Participants were distributed into 2 groups based on their UPSIT scores with a score equal or less than 33 in males and 34 in females defining hyposmia62.
Results
UPSIT scores in the normosmic group ranged from 34 to 28 (n=29 (21 women), age range [22-73]). The hyposmic group had UPSIT scores ranging from 9 to 34 (n= 28 (21 women), age range: [22-72]). CPT scores were significantly correlated with the UPSIT score (ρ=0.377, P=0.004) in the whole group of participants. We found this correlation to be much stronger in the hyposmic group (ρ=0.702, P<0.001).
Conclusions
The CPT allows for distinction between normosmia and olfactory dysfunction with high sensitivity and specificity. CPT scores are significantly correlated to UPSIT and Sniffin Sticks scores, especially in a group of individuals with olfactory dysfunction.
Acknowledgments
We thank Josiane Rivard for preparing the online questionnaire, Cécilia Tremblay, Émilie Aubry-Lafontaine and Frédérique Roy-Côté for data collection and the validation of the Chemosensory Perception Test, and all study participants and frontline healthcare workers facing the COVID-19 pandemic. This work was supported by Fonds de recherche du Québec – Santé (chercheur boursier junior 2 #283144 to JF). NB and JF had full access to all the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. FGL is the recipient of a tier-2 Canada research Chair. All authors declare no conflict of interest.
References




