
Abstract
Introduction Maternal underweight and obesity are prevalent conditions, associated with chronic, low-grade inflammation, poor fetal development, and long-term adverse outcomes for the child. The placenta senses and adapts to the pregnancy environment in an effort to support optimal fetal development. However, the mechanisms driving these adaptations, and the resulting placental phenotypes, are poorly understood. We hypothesised that maternal underweight and obesity would be associated with increased prevalence of placental pathologies in term and preterm pregnancies.
Methods Data from 12,154 pregnancies were obtained from the Collaborative Perinatal Project, a prospective cohort study conducted from 1959 to 1974. Macro and microscopic placental pathologies were analysed across maternal prepregnancy body mass index (BMI) to assess differences in the presence of pathologies among underweight, overweight, and obese BMI groups compared to normal weight reference BMI at term and preterm. Placental pathologies were also assessed across fetal sex.
Results Pregnancies complicated by obesity had placentae with increased fetal inflammation at preterm, and increased inflammation of maternal gestational tissues at term. In term pregnancies, increasing maternal BMI associated with increased maternal vascular malperfusion (MVM), odds of an appropriate mature placenta for gestational age, and placental weight, and decreased placental efficiency. Male placentae, independent of maternal BMI, had increased inflammation, MVM, and placental efficiency than female placentae, particularly at term.
Discussion Maternal underweight and obesity are not inert conditions for the placenta, and the histomorphological changes driven by suboptimal maternal BMI may serve as indicators of adversities experienced in utero and potential predictors of future health trajectories.
Introduction
Maternal underweight and obesity are global health burdens; maternal underweight remains a persisting problem, and the prevalence of obesity in pregnancy continues to rise1-3. Both conditions have been associated with higher levels of inflammation in the mother, which favour increased inflammation in the placenta4, suboptimal nutrient availability to the fetus4, and adverse pregnancy and offspring outcomes5,6. Yet, the mechanisms that drive these outcomes remain poorly understood.
The placenta is a critical regulator of the fetal environment and can adapt to mitigate harmful exposures, or maladapt to permit their adverse effects7. For example, inflammation can reduce placental area8 and impair spiral artery remodelling9, which can affect nutrient and gas exchange8-11 with potential consequences for the developing offspring12-14. Additionally, there is some evidence that maternal underweight and obesity may be unfavourable for placental development. Maternal obesity has been associated with chronic villitis15,16, both delayed and accelerated placental villous maturation16, and increased atheromas and villous infarcts16,17, pathologies which have been linked to placental insufficiency18, fetal growth restriction, and neurodevelopmental impairment16. The effects of maternal undernutrition or low BMI on placental pathologies are less well documented19. Animal models of undernutrition have shown evidence of abnormal placental vasculature and decreased fetal blood space, labyrinth and junctional zone area19, which may impair placental transfer20. The pro-inflammatory state induced by maternal underweight and obesity may also directly influence placental function, such as altered expression of placental nutrient transporters21-23. Therefore, it is important to understand even subtle placental phenotypes in these common conditions, as placental structural and functional adaptations may serve as a record of adversities experienced in utero, and could help reveal the mechanisms through which these adversities affect the developing offspring. However, the placental morphological and histopathologic changes induced by maternal underweight and obesity, in the absence of other major comorbidities or adverse perinatal events, are poorly characterized.
We hypothesised that, compared to women of normal weight, maternal underweight and obesity prepregnancy would be associated with increased prevalence of placental pathologies in term and preterm pregnancies, and that there would be differences in pathology prevalence based on placental sex. Using data from the Collaborative Perinatal Project (CPP), our primary objective was to determine whether placental pathologies were more prevalent in term and preterm pregnancies complicated by suboptimal maternal prepregnancy BMI. Our findings help to quantify placental pathologies in common pregnancy conditions, and uncover the mechanisms linking poor maternal metabolic health with suboptimal fetal growth and development.
Methods
Study design and population
Secondary data analysis was conducted using data from the CPP, a prospective cohort study designed to identify relationships between pregnancy and perinatal risk factors and child outcomes (https://catalog.archives.gov/id/606622). The CPP was conducted from 1959 to 1974 at 12 hospitals across the United States, and collected pregnancy data through the prenatal period and delivery, and child outcomes for approximately 58,000 pregnancies24.
The primary exposure of interest was maternal prepregnancy BMI, specifically maternal underweight, overweight, and obesity compared to normal weight as the reference category. BMI was classified according to the World Health Organization and American College of Obstetricians and Gynecologists guidelines, where maternal BMI is categorized as underweight (<18.5), normal weight (18.5–24.9), overweight (25–29.9), or obese (≥30). To evaluate the associations between maternal BMI and placental pathologies, the study sample was restricted to pregnancies with placental pathology data available, and maternal height and prepregnancy weight available to calculate maternal prepregnancy BMI. We included only singleton births from first pregnancies (parity and gravidity of zero), where fetal sex was documented as male or female. Gestational age below 24 weeks or above 43 weeks were excluded based on the limit of viability25 and morphological changes to the placenta such as those induced by cellular senescence26, and increased risk for fetal complications in post-term pregnancies27. The CPP calculated gestational age based on the last menstrual period to the nearest week. These selection criteria resulted in a sample of 12,154 pregnancies (Supplementary Figure 1).
Placental pathologies
The primary outcomes were macroscopic and microscopic placental pathologies (Figure 1). Macroscopic data included placental weight, largest and smallest diameter, thickness, and placental shape. Infant birthweight to placental weight/largest diameter/smallest diameter/thickness ratios were calculated as potential predictors of placental efficiency28,29. The top and bottom 0.5% of raw infant and placental anthropometry data (birthweight, placental weight, and placental dimensions) were excluded to remove biologically implausible data. The umbilical cord was assessed for cord edema and number of vessels, given the increased incidence of a single artery cord with gestational diabetes mellitus (GDM)30, a covariate of interest for pregnancies with obesity. Thrombosed fetal vessels and cut surface infarcts were assessed, which may be associated with impaired placental perfusion31. For microscopic variables: decidual vessel fibrinoids and atheroma were included, features of malperfusion32. Neutrophilic infiltration of the umbilical vein, umbilical artery, cord substance, chorion and amnion membranes, and chorion and amnion of the (fetal side) placental surface were also obtained, which may be indicative of ascending maternal infection33. Cut surface calcification was included as an indicator for placental maturation34. Syncytium-nuclear clumping, or syncytial knots, and stromal fibrosis are signs of accelerated villous maturation and were thus included35. Prescence of Langhans’ layer, Hofbauer cells, and pathological edema were included as indicators of placental immaturity36,37. A variable provided for the apparent maturity of the placenta was also included as a marker for appropriate placental development for gestational age. For multivariable analyses, categorical placental pathology variables were collapsed into binary categories (Supplementary Table 1).

The presence or absence of categorical placental pathologies across maternal body mass index (BMI) groups, where mothers were categorized as underweight (UW), normal weight (NW), overweight (OW) or having obesity (OB) by prepregnancy BMI, in term (n=10,415; panel A) and preterm (n=1,739; panel B) pregnancies.
We derived additional summary scores for placental inflammation, maternal vascular malperfusion (MVM), and placental immaturity. A maternal inflammation summary score was derived from the following variables: opacity of membranes and neutrophil infiltration of the amnion and chorion membranes and of the placental surface. Where data were available for all constituent variables, the individual variable scores were summed to create a composite score ranging from zero to fourteen, where a higher score represents increased levels of inflammation. Similarly, a fetal inflammation summary score was derived from neutrophilic infiltration of the umbilical vein, artery, and cord substance to create a composite score from zero to nine. A summary score considering features of MVM was derived from: presence of infarcts and syncytium-nuclear clumping to create a score ranging from zero to two, where a higher score indicates increased MVM. A placental immaturity score was derived from the following variables: Langhans’ layer, Hofbauer cells, stromal fibrosis, and syncytium-nuclear clumping, to create a score ranging from zero to seven where a higher score indicates a more immature placental phenotype (Supplementary Table 2).
Maternal demographics
Our primary exposure of interest, maternal prepregnancy BMI, was defined based on measured height and self-reported prepregnancy weight collected at study enrollment. In addition to prepregnancy BMI, maternal demographic data including age, race, education, marital status, income, socioeconomic index, housing density, smoking history, diabetes mellitus status, and gestational weight gain were obtained. The socioeconomic index is a composite numerical index derived from scores for education (of the head of household/chief earner), occupation (of the head of household/chief earner), and family income, ranging from 0.0-9.5, where 9.5 represents the highest socioeconomic status38. Smoking history was provided as the number of cigarettes smoked per day at the time of the interview, from zero cigarettes (including non-smokers) to 60 cigarettes per day. Additional smoking categories included 61 or more cigarettes per day, regular smoker but less than one cigarette per day, and irregular smoker but less than four cigarettes per month. Smoking history was presented as non-smokers (including women currently smoking zero cigarettes per day), light smokers (less than one pack of 20 cigarettes per day), and heavy smokers (one or more packs of 20 cigarettes per day). Diabetes mellitus was presented as presence or absence, where presence included diabetes mellitus reported before pregnancy, during pregnancy, both before and during, during and postpartum, or before, during, and postpartum. Based on current recommendations from the Institute of Medicine (IOM) guidelines (2009), maternal weight gain was categorized as inadequate, adequate, or excessive for singleton pregnancies based on prepregnancy BMI, where the recommended weight gain ranges are 28–40 pounds, 25–35 pounds, 15–25 pounds or 11–20 pounds39 for mothers who are underweight, normal weight, overweight, or have obesity, respectively.
Statistical analyses
Univariate analyses
Univariate analysis was conducted to evaluate differences in the prevalence of placental pathologies across maternal prepregnancy BMI groups. Given that the presence of some placental pathologies are dependent on gestational age40, we conducted all analyses stratified for term and preterm placentae. Differences between maternal BMI groups and placental measures were determined by Kruskal–Wallis test with Steel–Dwass post hoc for continuous nonparametric data, and Likelihood Ratio Chi Square test for categorical data. Placental pathologies were also assessed across fetal sex. Data are presented as median (interquartile range) and Wilcoxon test effect size (r) (95% confidence interval; CI) for non-parametric continuous data, and frequency (percentage) and Cramer’s V effect size (95% CI) or odds ratio (95% CI) (for binary fetal sex analyses) for categorical variables. Statistical significance was defined as p<0.05 and all tests were two-sided. Data were analysed using JMP statistical software (14.0), and Wilcoxon test effect size and Cramer’s V effect size were calculated in R (4.1.2).
Multivariable analyses
We performed multivariable logistic and linear regression to determine the relationships between maternal prepregnancy BMI and placental pathologies at term and preterm. Logistic regression models were used to determine the associations between maternal BMI (continuous) and binary placental pathologies. Categorical placental pathology variables were collapsed into binary categories to calculate odds ratios for the pathological phenotype. Any data coded as unknown, unable to determine, or missing were excluded from regression analyses. Data are presented as unadjusted (OR) or adjusted units odds ratio (aOR) (95% CI). Linear regression models were used to determine the associations between maternal BMI (continuous) and continuous placental pathology variables. Data are reported as adjusted beta coefficient (aβ) (95% CI). Covariates of interest were identified a priori and included fetal sex (male/female), maternal race (White, Black, and Other), maternal age (continuous), smoking history (non-smoker, light smoker, heavy smoker), maximum gestational weight gain (continuous), diabetes (yes/no), maternal education (continuous), and socioeconomic index (continuous). Two regression models were defined a priori: 1) An unadjusted model was first used to identify the associations between prepregnancy BMI alone (as a continuous variable) with placental pathologies and 2) an adjusted model adjusted for the covariates defined above.
Results
Maternal demographics differed across maternal BMI groups
Maximum gestational weight gain among preterm (Wilcoxon test effect size, r=-0.09 [-0.14 to -0.04]) and term (r=-0.05 [-0.07 to -0.03]) pregnancies was greatest in underweight and lowest in obese BMI groups (Supplementary Tables 3-4). However, according to IOM (2009) guidelines, weight gain in underweight pregnancies was still inadequate at preterm and term, while most pregnancies with obesity had either inadequate or excessive weight gain at preterm, and excessive weight gain at term (Supplementary Tables 3-4). Maternal age, race, education, marital status, income, socioeconomic index, and housing density also differed by BMI group (Supplementary Tables 3-4).
Maternal obesity associated with increased neutrophil infiltration of gestational tissues
Among preterm pregnancies, fetal inflammation, characterised by the composite fetal inflammation summary score, was greater in placentae from mothers with obesity compared to underweight and normal weight BMI groups (r=0.009 [-0.04 to 0.06], Table 1). There were no effects of maternal BMI group on neutrophil infiltration in the preterm membranes or placental surface. Neutrophil infiltration of the umbilical vein (aOR=1.06 [1.01–1.12]), umbilical cord substance (aOR=1.08 [1.02– 1.14]), and amnion membrane (OR=1.05 [1.01–1.10]), but not the umbilical artery, chorion membrane, or amnion and chorion of the placenta, were more likely with increasing maternal BMI (Table 2).
Associations between maternal prepregnancy BMI and microscopic placental pathologies in preterm pregnancies, N=1739.
Multivariable analyses for associations between maternal prepregnancy BMI (continuous) and microscopic placental pathologies in preterm pregnancies, N=1739.
Among term pregnancies, pregnancies complicated by obesity had the greatest percentage of marked neutrophil infiltration of the umbilical vein and artery, amnion and chorion membranes, and amnion, but not chorion, of the placental surface (Table 3). The maternal inflammation summary score was greatest among pregnancies complicated by obesity, though there were no differences between BMI groups on post hoc analysis (r=0.008 [-0.01 to 0.03], Table 3). Further, neutrophilic infiltration of the umbilical vein (aOR=1.03 [1.01–1.05]), artery (aOR=1.04 [1.00–1.07]), and cord substance (aOR=1.04 [1.01–1.07]) increased with increasing BMI (Table 4). Neutrophil infiltration of the amnion membrane (aOR=1.06 [1.03–1.08]), chorion membrane (aOR=1.04 [1.02–1.06]), amnion of the placental surface (aOR=1.04 [1.01–1.07]), and chorion of the placental surface (aOR=1.04 [1.02–1.06]) were also greater with increasing BMI (Table 4).
Associations between maternal prepregnancy BMI and microscopic placental pathologies in term pregnancies, N=10,415.
Multivariable analyses for associations between maternal prepregnancy BMI (continuous) and microscopic placental pathologies in term pregnancies, N=10,415.
Higher maternal BMI associated with MVM among term pregnancies
At term, increasing maternal BMI was associated with greater odds of an appropriately mature placenta based on apparent maturity of the placenta (aOR=0.94 [0.92–0.97]) and increased MVM (aβ=0.007 [0.004–0.01], Table 4), and placentae from mothers with obesity had the greatest percentage of thrombosed fetal vessels compared to all other BMI groups (Cramer’s V=0.03 [0.004–0.05], Supplementary Table 5). Additionally, presence of infarcts alone was more likely as maternal BMI increased (aOR=1.03 [1.02–1.05], Supplementary Table 6). There were no differences in apparent placental maturity or vasculature-related pathologies by BMI among preterm pregnancies (Table 1).
Both maternal underweight and increased BMI influenced placental anthropometry
In preterm pregnancies where mothers were underweight, placental weight was reduced compared to placentae from mothers with overweight and obesity (r=0.04 [-0.004–0.09]), and smallest diameter was reduced compared to placentae from pregnancies complicated by obesity (r=0.06 [0.01–0.11], Supplementary Table 7), but there were no differences in placental anthropometry compared to normal weight BMI. Among term pregnancies where mothers were underweight, placental weight (r=0.08 [0.06–0.10]) and smallest diameter (r=0.05 [0.03–0.07]) were reduced compared to all other BMI groups, with most prominent differences between the underweight and obese groups (Supplementary Table 5). At term only, birthweight to placental weight ratio was higher in mothers who were underweight compared to overweight, but not different than normal weight (r=-0.03 [-0.05 to -0.006], Supplementary Table 5). Similarly, when considering BMI as a continuous variable, placental weight and smallest diameter increased with increasing maternal BMI among preterm and term pregnancies, and birthweight to placental weight ratio decreased with increasing maternal BMI at term (Supplementary Tables 6,8).
Fetal sex influenced placental pathology
Among preterm pregnancies, female placentae had a greater fetal inflammation summary score than male placentae (r=-0.05 [-0.10 to - 0.004], Table 5), but there were no sex differences in neutrophil infiltration of the membranes or placental surface. Male term placentae had greater fetal and maternal placental inflammation, including neutrophil infiltration of the umbilical vein, umbilical cord substance, amnion membrane, chorion membrane, amnion of the placenta, chorion of the placenta, and fetal and maternal inflammation summary scores (Table 5). Further, when considering only pregnancies with maternal obesity, at term, male placentae had greater neutrophil infiltration of the umbilical vein and chorion membrane than female placentae (Supplementary Figure 2). Female preterm placentae had increased syncytium-nuclear clumping (OR=0.53 [0.31–0.91], Table 5), but there were no differences in presence of infarcts or MVM summary score between sexes preterm. Male term placentae had increased MVM (r=0.04 [0.02–0.06], Table 5) and placental infarcts compared to female placentae (OR=1.22 [1.11–1.33], Table 6). Infant birthweight to placental weight ratio was also increased in males compared to females at preterm (r=0.07 [0.03–0.12]) and term (r=0.07 [0.05–0.09], Table 6).
Associations between fetal sex and microscopic placental pathologies in preterm (N=1739) and term (N=10,415) pregnancies.
Associations between fetal sex and macroscopic placental pathologies in preterm (N=1739) and term (N=10,415) pregnancies.
Discussion
We evaluated the associations between maternal prepregnancy BMI and the prevalence of placental pathologies in preterm and term pregnancies, to better understand the placental mechanisms that may explain poor pregnancy and offspring outcomes in pregnancies complicated by suboptimal maternal BMI. Using data from 12,154 pregnancies from the Collaborative Perinatal Project, we found placental inflammation was increased in pregnancies complicated by maternal obesity, and notably, the inflammatory response was different based on gestational age. Maternal obesity also associated with increased MVM of the placenta, and increased maternal BMI associated with greater odds of having an appropriate mature placenta at term. Placental efficiency was highest in pregnancies where mothers were underweight and in male placentae, and pathologies also differed by fetal sex. Suboptimal maternal BMI thus alters normal gestational tissue development, with likely effects on function.
The inflammatory conditions established by maternal obesity may favour placental inflammation. In support of this, we found that higher maternal BMI associated with increased fetal (e.g. neutrophilic infiltration of the umbilical vein, artery, and cord substance) inflammation at preterm, and maternal (e.g. neutrophilic infiltration of the amnion and chorion membranes, amnion and chorion of the placenta, and opacity of membranes) gestational tissue inflammation at term. While few studies have characterised fetal- and maternal-specific placental inflammation in the context of both maternal BMI and gestational age, at term, maternal inflammation has been previously characterized in pregnancies with obesity, evidenced by increased pro-inflammatory cytokines in the placenta41, and increased maternal, but not fetal, inflammatory lesions17,42. Other studies have found no differences in placental inflammation by maternal BMI in term pregnancies, however, these cohorts had a small number of cases43,44. Less is known about the relationships between maternal obesity and specific placental inflammation at preterm, however, maternal obesity has been associated with greater risk of chorioamnionitis leading to preterm birth45, and a combination of maternal (defined as inflammation in the chorion, amnion, and decidua) and fetal (inflammation of the umbilical cord and chorionic plate fetal vessels) gestational tissue inflammation has been linked to higher risk of extreme preterm birth than maternal gestational tissue inflammation alone46. In the context of ascending infection, fetal placental inflammation of the umbilical cord has been associated with greater neonatal morbidity and mortality, particularly among preterm pregnancies, than maternal placental inflammation47-49. Our study, unlike many others, considers both suboptimal maternal BMI and gestational age, and suggests that increased maternal BMI associates with fetal placental inflammation at preterm, which has been linked to adverse pregnancy and offspring outcomes50,51, and maternal focused placental inflammation at term. Fetal inflammation of the placenta at preterm could thus be an important risk factor for adverse offspring outcomes, and maternal placental inflammation, though less frequently associated with clinical correlates50, nonetheless suggests that suboptimal maternal BMI alters gestational tissue histomorphology.
Interestingly, preterm female placentae had increased fetal inflammation, while term male placentae had increased fetal and maternal inflammation. Male placentae have been observed to have higher rates of chronic inflammatory lesions in extreme preterm pregnancies52, chronic deciduitis among extreme preterm pregnancies with pre-eclampsia and intrauterine growth restriction53, and enrichment in inflammatory pathways54. Fewer studies have observed increased female placental inflammation compared to males, however, female placentae have been shown to have increased chronic villitis in pregnancies complicated by maternal obesity, although those observations were restricted to pregnancies at or near term15, and increased expression of genes related to immune regulation in normal, term pregnancies55. Our findings suggest that male placentae are more susceptible to inflammation in term pregnancies, which could increase risk for impaired growth or neurodevelopment and long term health outcomes56,57, while increased fetal inflammation among preterm female placentae warrants further investigation. Given the associations of maternal obesity and male sex with increased placental inflammation, term males born to mothers with obesity may be most susceptible to placental inflammation. To further investigate this, we conducted an exploratory analysis to assess whether fetal sex associated with placental inflammation among pregnancies with obesity alone. Increased odds of inflammation in male placentae at term only, though not to the same extent as BMI inclusive differences, suggests that both maternal obesity and male sex may be independent risk factors for placental inflammation at term. Further studies are needed to corroborate this finding.
We found MVM also associated with increased maternal BMI among term pregnancies, consistent with existing data58. Previous studies have documented increased maternal vascular lesions44 and decidual vasculopathy, but no other lesions associated with MVM, in placentae from term pregnancies complicated by obesity compared to normal weight, although this was attributed to maternal hypertensive disease15. MVM lesions impair intervillous blood flow, altering oxygen and nutrient delivery to the fetus32, and are associated with adverse offspring outcomes, including preterm birth, intrauterine growth restriction, and small for gestational age infants32. Our findings suggest that the adverse environment established by maternal obesity may impair the development and function of placental vasculature, and thus fetal development. Despite known associations of MVM and preterm birth32,59, increased BMI associated with MVM only among term pregnancies in our cohort15,32,44, suggesting the importance of vascular pathologies across gestation in pregnancies complicated by maternal obesity. Further, male placentae had increased MVM lesions compared to females at term in our study, consistent with other findings of increased decidual vasculopathy in males15. Thus, placental vasculature pathology may not be so severe as to result in early pregnancy or other adverse perinatal events, but may still have long term implications for the infant.
In contrast to previous studies, we found increased maternal BMI associated with greater odds of having an appropriately mature placenta at term. Placentae from women with obesity have been shown to have immaturity of the villous tree compared to women of normal weight43, suggesting structural and functional maladaptation of the vasculature or decreased efficiency in maternal-fetal exchange43. We did, however observe other placental vascular pathologies, evidenced by increased MVM with higher maternal BMI. Placental maturity was classified by CPP pathologists as placental appearance of <20, 20–27, 28–36, or ≥37 weeks’ gestation, based on presence of fibrin under the chorionic plate, presence of cysts on the cut surfaces, lack of Langhans layer, relative uniformity of villous size, crowded fetal capillaries within villi, and increased frequency of syncytial knots. In addition to the lower number of cases of obesity in our cohort relative to the current rates, changes to criteria used to diagnose distal villous immaturity, which was only introduced after the time of the CPP60, may in part account for these differences in apparent placental maturity. Overall, a consistent, universal classification of placental maturation disorders would be beneficial in reducing variation in assessment of placental maturity across studies61.
Our findings of decreased placental size and increased infant birthweight to placental weight ratio with lower maternal BMI are consistent with reduced nutrient availability in underweight pregnancies5,20,62, and suggest that the placenta may adapt to increase nutrient delivery to the fetus, whereas placentae from higher BMI pregnancies may adapt by regulating nutrient transfer to the fetus in the face of sufficient or overabundance of nutrients63,64. Conversely, among term pregnancies, decreased birthweight to placental smallest diameter ratio with lower maternal BMI could suggest lower placental efficiency in pregnancies with underweight. However, placental diameter is reflective of the lateral growth of the placenta and area of the uterine lining that it encompasses, and may be influenced by inter-individual variations such as differences in placental shape, whereas placental weight captures multiple dimensions of placental growth65. Further, males had higher birthweight to placental size ratios in both preterm and term pregnancies, consistent with previous studies66, suggesting greater placental efficiency than females. Male fetuses tend to grow more rapidly than females and invest greater resources in growth than placental development and reserve capacity55,67-69, and as a result, may be more susceptible to placental insults as well as adverse later health outcomes67. Sex-based differences in fetoplacental growth and development may be attributed to a number of contributing biological factors, including X chromosome inactivation68,70, sex-specific response to glucocorticoids68,71, and levels of sex hormones68. Taken together, our results may suggest that males born to mothers who are underweight have the greatest placental efficiency, particularly at term.
Strengths of our study included the large population-based cohort, where previous studies have been limited to animal models of maternal malnutrition or inflammation to assess placental histopathology, or have lacked population size and comprehensive data. Importantly, the large sample size, collection of socioeconomic and demographic factors, deep phenotyping, and prospective nature of the dataset enables a thorough investigation of the relationships between maternal BMI and placental pathologies in a diverse population. Yet, due to the cohort’s historical nature, a limitation of our study is that the prevalence of obesity was lower than current rates; only 2.63% of our cohort were classified as having obesity prepregnancy, compared to 29% of American women currently72. Rates of smoking were also increased during the time of the study compared to rates today (42-45% during the time of CPP data collection73 compared to 16% in 201974), and no data were collected on maternal alcohol consumption75. Additionally, no data were provided for GDM specifically, which is associated with adverse pregnancy outcomes and is comorbid with obesity76,77, however, rates of GDM were much lower during the time of the study than current rates (0.3% in 197978 compared to 7.6% from 2007-201479), so any confounding is likely to be minimal. Placental pathology was not re-assessed, however, definitions of pathologies were largely consistent between the CPP and current Amsterdam Placental Workshop Group Consensus Statement criteria18, particularly for our variables of interest. Given the population-based design, our findings may still be applicable to a broad and diverse population today, due to the large sample size and thorough collection of demographic and placental pathology data.
Our data demonstrate that compared to normal weight, maternal underweight and obesity prepregnancy, even in the absence of other significant pregnancy complications, are not inert conditions for the developing placenta16,80, which may have consequences not only for immediate pregnancy and fetal outcomes but postnatal growth and health trajectories28,29,81,82. Characterising placental (mal)adaptations to common maternal conditions using clinically-relevant indicators can help understand the mechanisms through which these conditions affect the developing offspring, and aid clinical decision making to better support high-risk pregnancies and inform interventions to optimise pregnancy, placental, and infant health.
Data Availability
The data that support the findings of this study are available in the United States National Archives at https://www.archives.gov/research/electronic-records/nih.html, National Archives Identifier: 606622 (Record Group 443: Records of the National Institutes of Health [NIH]). Derived data supporting the findings of this study are available from the corresponding author on request.
https://www.archives.gov/research/electronic-records/nih.html
Funding and Competing Interests
The authors have no competing interests to declare. This research is funded by the Faculty of Science, Carleton University. HS was supported by a Mitacs Research Training Award. KLC is supported by grants from the Canadian Institutes of Health Research, Natural Sciences and Engineering Research Council of Canada, the Molly Towell Perinatal Research Foundation (New Investigator), and Carleton University Office of Research.
Author Contributions
Conceptualization, methodology: HS, KLC, DG, LNA; formal analysis: HS; writing—original draft preparation: HS, KLC; writing—review and editing: HS, KLC, DG, LNA; visualization: HS, KLC.
Supplementary tables
Binary categories for placental pathology variables for multivariable analysis.
Derived summary scores variable coding.
Maternal characteristics by prepregnancy BMI in preterm pregnancies, N=1739.
Maternal characteristics by prepregnancy BMI in term pregnancies, N=10,415.
Associations between maternal prepregnancy BMI and macroscopic placental pathologies in term pregnancies, N=10,415.
Multivariable analyses for associations between maternal prepregnancy BMI (continuous) and macroscopic placental pathologies in term pregnancies, N=10,415.
Associations between maternal prepregnancy BMI and macroscopic placental pathologies in preterm pregnancies, N=1739.
Multivariable analyses for associations between maternal prepregnancy BMI (continuous) and macroscopic placental pathologies in preterm pregnancies, N=1739.
Supplementary figures

Participant flow selection and placental pathologies of interest.

{kind=link}
{kind=link}
{kind=link}
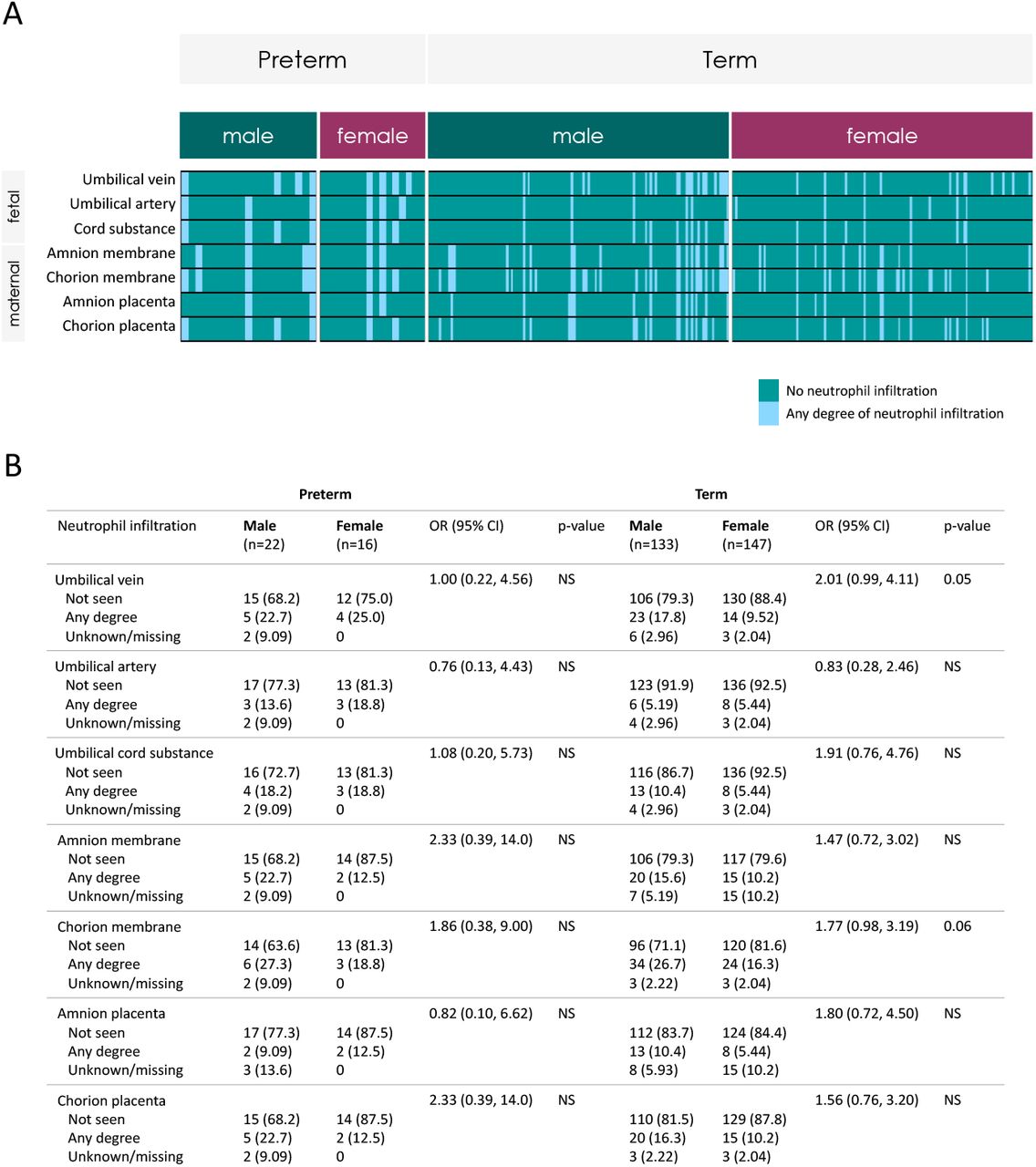
Placental neutrophil infiltration in pregnancies with maternal obesity by fetal sex, n=318. Prescence or absence of neutrophil infiltration for female and male placentae among pregnancies with maternal obesity by preterm (male: n=22, female: n=16) and term (male: n=133, female: n=147) birth. Data are n (%) (Likelihood Ratio Chi Square test) and odds ratio (95% CI) for presence of pathology in male placentae.
Acknowledgments
The authors thank the U.S. National Archives for the publicly available Collaborative Perinatal Project data, and Marina White for her assistance with obtaining the dataset.
References
- 1.↵
- 2.
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.
- 11.↵
- 12.↵
- 13.
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.↵
- 82.↵




