
ABSTRACT
Background Inequities in the burden of COVID-19 observed across Canada suggest heterogeneity within community transmission.
Objectives To quantify the magnitude of heterogeneity in the wider community (outside of long-term care homes) in Toronto, Canada and assess how the magnitude in concentration evolved over time (January 21 to November 21, 2020).
Design Retrospective, population-based observational study using surveillance data from Ontario’s Case and Contact Management system.
Setting Toronto, Canada.
Participants Laboratory-confirmed cases of COVID-19 (N=33,992).
Measurements We generated epidemic curves by SDOH and crude Lorenz curves by neighbourhoods to visualize inequities in the distribution of COVID-19 cases by social determinants of health (SDOH) and estimated the crude Gini coefficient. We examined the correlation between SDOH using Pearson correlation coefficients.
Results The Gini coefficient of cumulative cases by population size was 0.41 (95% CI: 0.36-0.47) and were estimated for: household income (0.20, 95%CI: 0.14-0.28); visible minority (0.21, 95%CI: 0.16-0.28); recent immigration (0.12, 95%CI: 0.09-0.16); suitable housing (0.21, 95%CI: 0.14-0.30); multi-generational households (0.19, 95%CI: 0.15-0.23); and essential workers (0.28, 95% CI: 0.23-0.34). Most SDOH were highly correlated.
Locally acquired cases were concentrated in higher income neighbourhoods in the early phase of the epidemic, and then concentrated in lower income neighbourhoods. Mirroring the trajectory of epidemic curves by income, the Lorenz curve shifted over time from below to above the line of equality with a similar pattern across SDOH.
Limitations Study relied on area-based measures of the SDOH and individual case counts of COVID-19. We cannot infer concentration of cases by specific occupational exposures given limitation to broad occupational categories.
Conclusion COVID-19 is increasingly concentrated by SDOH given socioeconomic inequities and structural racism.
Primary Funding Source Canadian Institutes of Health Research.
INTRODUCTION
Inequities in the burden of COVID-19 were observed early in Canada(1) and around the world,(2-4) suggesting that racialized and economically marginalized communities faced disproportionate risks of acquisition.
Descriptive data suggested a temporal shift in how SARS-COV-2 may have spread through transmission networks over a short period of time within cities.(5, 6) For example, in the Greater Toronto Area, Canada, (population over 7 million)(7) the first wave from January to August, 2020 quickly divided into micro-epidemics in congregate settings (e.g., long-term care homes) and what seemed to be more diffuse spread in the wider community.(6) However, an examination of cumulative cases suggested considerable heterogeneity within the wider community with greater risks associated with household size and occupation.(8)
Heterogeneity is an established marker of inequities, with the application of Lorenz curves and Gini coefficients increasingly used to quantify and compare health inequities(9) in infectious diseases.(10-12) Health inequities, in turn, represent unmet prevention needs acting as mechanistic drivers of onward transmission in epidemics.(13, 14) Specifically, observed cases concentrated within a smaller subset of the population which often indicates disproportionate risks of onward transmission, whether at the individual-level mediated via higher contact rates(13, 14) or more commonly, at the network-level such as household density or high-exposure occupations.(8, 15)
Gini coefficients have been commonly used in sexually transmitted infections as a measure of spatial concentration to help identify spatial ‘core-groups’ that experience disproportionate risks in the context of core-group theory.(10, 11) Core-group theory is based on the premise that if prevention efforts are not effective within a smaller group of people experiencing very high risks of both acquisition and onward transmission, the epidemic cannot be controlled (10, 11). In addition to sexually transmitted infections, Lorenz curves and Gini coefficients have been used for a range of other health outcomes.(16-19) For example, inequities in longevity over time,(18) oral health,(17) and premature mortality(20) have been examined against income-levels, and more recently inequities in health outcomes have been examined across other social determinants, including unemployment.(16)
The present study’s overarching objective is to improve our understanding of the role of social determinants in shaping SARS-CoV-2 transmission dynamics in Toronto, the largest city and economic capital of Canada. Specifically, we first quantified the magnitude of heterogeneity in the wider community (outside of long-term care homes) by comparing the concentration of cases by area-level social determinants. Second, we assessed how the magnitude in concentration of COVID-19 cases evolved from January to November, 2020.
METHODS
Study design, setting, and population
We conducted a retrospective, population-based observational study using routinely collected surveillance data; reported according to the STROBE (reporting of observational studies) guidelines.(21) The study population comprised the City of Toronto (population 2,731,571).(22) The study period included cases with a January 21 (first documented case was reported on January 23, 2020)(23) to November 21, 2020 episode date. The episode date is either the date of symptom-onset as self-reported by individuals, or the test-submission date in cases where symptom data are either missing or individuals were asymptomatic.(24) We excluded individuals residing in long-term care homes because congregate settings represent a different epidemic setting from the wider community. Our unit of analysis was the census geographic unit of the dissemination area (DA), which represents on average 400-700 residents.(25)
Data sources
We used Ontario’s Case and Contact Management (CCM+) surveillance system of person-level, anonymized, surveillance data which includes information on laboratory-confirmed cases by episode date, reported date, the DA of residence, and demographic, exposure, and setting-specific characteristics (e.g., -long-term care residence). The DA of residence was determined using the Postal Code Conversion File version-SLI.(26)
For DA-level variables on the social determinants, we used publicly available data from the 2016 Canadian Census,(27) and two variables that were not publicly available: after-tax, per-person equivalent income ranking across DAs within the Toronto which was obtained from ICES (a not-for-profit research institute that securely houses Ontario’s health-related data); and a measure of multi-generational households which was curated by and sourced from the Ontario Community Health Profiles Partnership.(28)
Measures
For social determinants, we considered measures previously shown to be associated with test-positivity;(29) and mechanistically drive transmission dynamics by considering frequency of contacts and who contacts whom.(30) These include:
socio-demographic indicators that are proxies of economic barriers and systemic racism (income; % visible minority; % recent immigration);
dwelling-related variables (% suitable housing;(31, 32) % multi-generational households); and
occupation-related variables (% working in essential services [health; trades, transport and equipment operation; sales and services; manufacturing and utilities; resources, agriculture, and production])(33)
Details and definitions for each variable are included in Appendix Table A1.
Analyses
We generated crude Lorenz curves by DA to visualize inequalities in the distribution of confirmed SARS-CoV-2 cases. Lorenz curves are used to assess the relationship between two cumulative distributions: the cumulative proportion of diagnoses and the cumulative proportion of the population. This information can be summarized using the estimated crude Gini coefficient (the comparison of the cumulative proportion of population against the cumulative proportion of diagnoses) where a coefficient of zero represents complete equality and one represent complete inequality. We included all DAs in this analysis, including DAs without SARS-CoV-2 cases. We excluded cases with missing DA numbers that we were not able to link to DA level characteristics.
We examined the correlation between social determinants using Pearson correlation coefficients.(34) To investigate concentration of confirmed cases by social determinants, we first described the cumulative and daily epidemic curves by each social determinant. We then generated Lorenz curves using x-axes that represent the proportion of the population ranked by DA-level estimates of each value of the social determinant and subsequently estimated the crude Gini coefficient, over the entire study period and for each mutually exclusive time-period using the dates of large-scale restriction measures in Toronto: January to March 16 (pre-closure/shutdown); March 17 to May 18 (during shutdown and prior to stage 1 re-opening); May 19 to June 23 (stage 1); June 24 to July 30 (stage 2); July 31 to October 9 (stage 3); October 10 to November 21 (modified stage-2) (Appendix Table A2).(35) We generated 95% confidence intervals for the Lorenz curves and Gini coefficients using bootstrapping (9, 11).
All analyses were conducted in R (version 4.0.2), and spatial maps were generated using ArcGIS (version 10.7).
Ethics approval
The University of Toronto Health Sciences Research Ethics Board (protocol no. 39253) approved the study.
RESULTS
Between January 21 and November 21, 2020, there were N=33,992 observed cases of COVID-19, excluding long-term care residents (Appendix Figure A1). The median population size of a DA was 450 (interquartile range, 446-768, Appendix Table A3). Among 3,702 DAs in the City of Toronto, 404 DAs had zero reported cases, representing 10.9% of DAs and 8.1% of the population. Data on social determinants were missing in 0.51-0.57% of DAs (Table 1). The proportion of cases that were travel-acquired decreased over time: from 51% (pre-closure/shutdown) to 3% (during shutdown), 1% (stage 1), 5% (stage 2), 3% (stage 3), and 1% (modified stage-2).
Geographic concentration of cases
The overall Gini coefficient of cumulative cases by population size was 0.41 (95% CI: 0.36-0.47) (Figure 1A). For example, 53.7% (95% CI: 53.2-54.3%) of cumulative cases were diagnosed in 25% of the population, with the largest concentration of cases in the north-west part of the city (Figure 1B) which overlap with the social determinants under study (Appendix Figure A2).


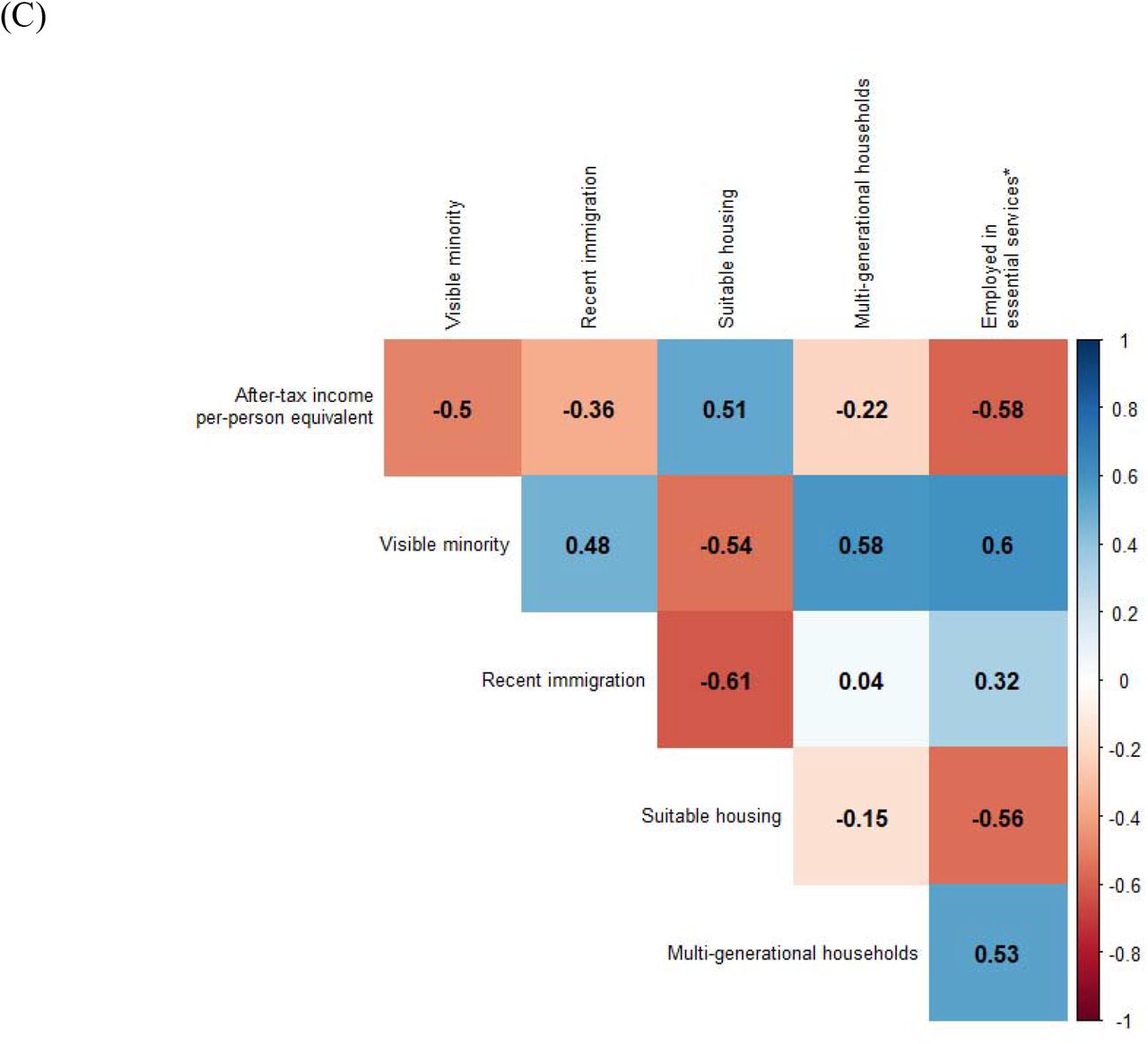
In Panel A, the Lorenz curve depicts the cumulative proportion of laboratory-confirmed diagnoses, excluding residents of LTCH, by the cumulative proportion of the population by dissemination-area. The dashed line represents the line of equality. For example, 53.7% (95% CI: 53.2%-54.3%) of cases were diagnosed among 25% of the population as shown by the dashed horizontal and vertical red lines. Panel B shows the map of lowest to highest deciles with respect to laboratory-confirmed diagnoses per capita by dissemination-area for the City of Toronto public health unit; and excluding cases among LTCH residents. Panel C depicts a heat map of the correlation between social determinants at the dissemination area, where 1 represents a perfect positive correlation and −1 represents a perfect negative correlation. LTCH: long-term care homes
Distribution and correlation of social determinants
At the DA-level, the median per-person equivalent after-tax income was $45,750 CAD per year; the median proportion residing in suitable housing was 92.6%; and the median proportion working in non-health essential services was 38.5% (Table 1). Table A4 shows the values of each social determinant across deciles.
The correlation matrix of social determinants suggests considerable overlap (Figure 1C). For example, DAs with the lowest income were correlated with a higher prevalence of essential services workers (correlation coefficient, −0.58) and, multigenerational households (correlation coefficient, −0.22), whereas higher-income DAs were correlated with a higher prevalence of suitable housing (correlation coefficient, 0.51).
Epidemic trajectory by social determinants
The epidemic curve of cumulative cases per 100,000 population, stratified by decile for each social determinant is shown for one variable from each category (household income, suitable housing, and essential services) in Figure 2. Results for the remaining three social determinants are presented in Appendix Figure A3. The daily rates are shown as deciles in Appendix Figure A4.
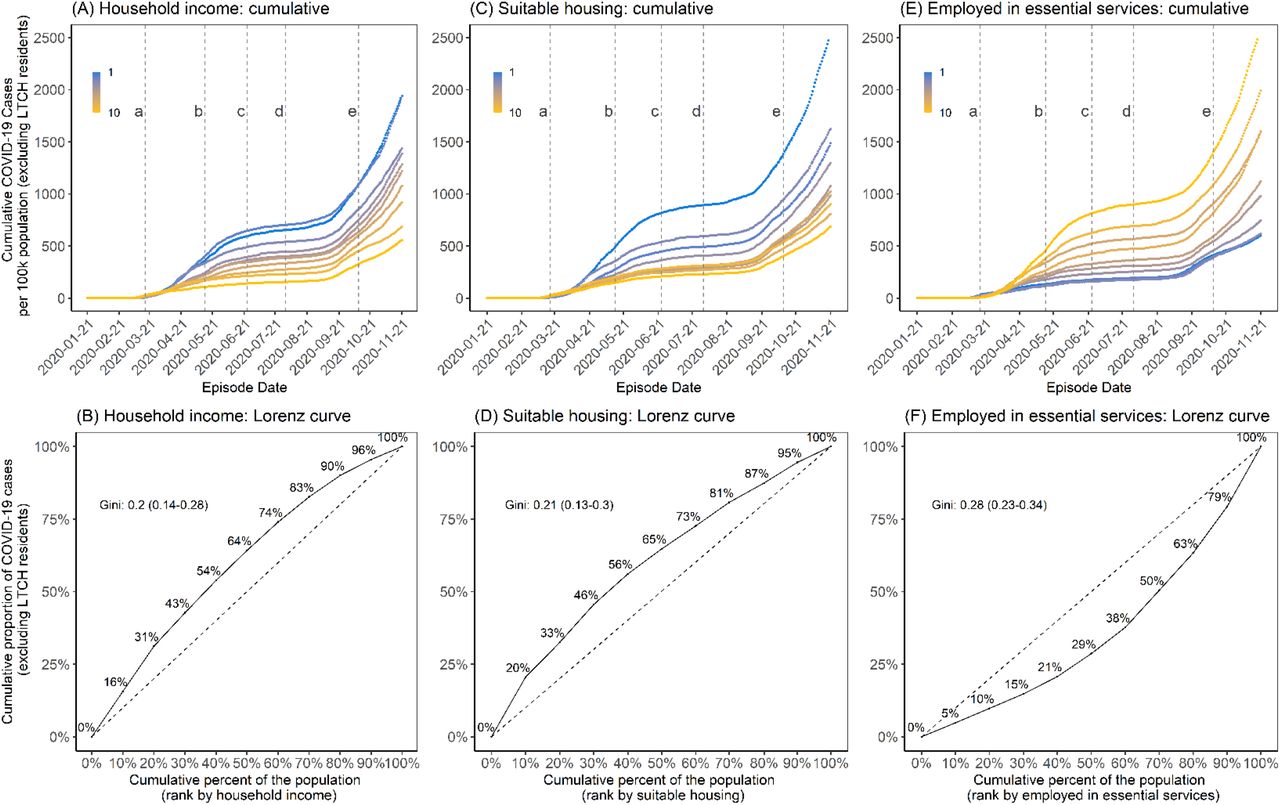
Panels A and B represent income (after-tax, per-person equivalent) deciles where the lowest decile (decile 1) represents the lowest income decile and decile 10 represents the highest income decile. Panels C and D represent suitable housing deciles where the lowest decile (decile 1) represents areas with the highest proportion of homes deemed suitable housing;(27) and the highest decile (decile 10) represents areas with the lowest proportion of homes deemed suitable housing.(27) Panels E and F represent essential services where the lowest decile represents DAs with the fewest essential workers and the highest decile (decile 10) represents the highest prevalence of individuals employed in essential services. The Lorenz curves (Panels B, D and F) depict the concentration of cases by each determinant and the dashed line represents the line of equality; for example, 30% of the population residing in the lowest income areas account for 42.7% (95% CI: 42.2%-43.3%) of cumulative cases (Panel B). The time-periods are: (a) March 17, 2020, start of shutdown; (b) May 14, 2020, start of stage 1 re-opening; (c) June 24, 2020, start of stage 2 re-opening; (d) July 31, 2020, start of stage 3 re-opening; and (e) October 10, 2020, start of modified stage 2. DA: dissemination area; LTCH: long-term care homes
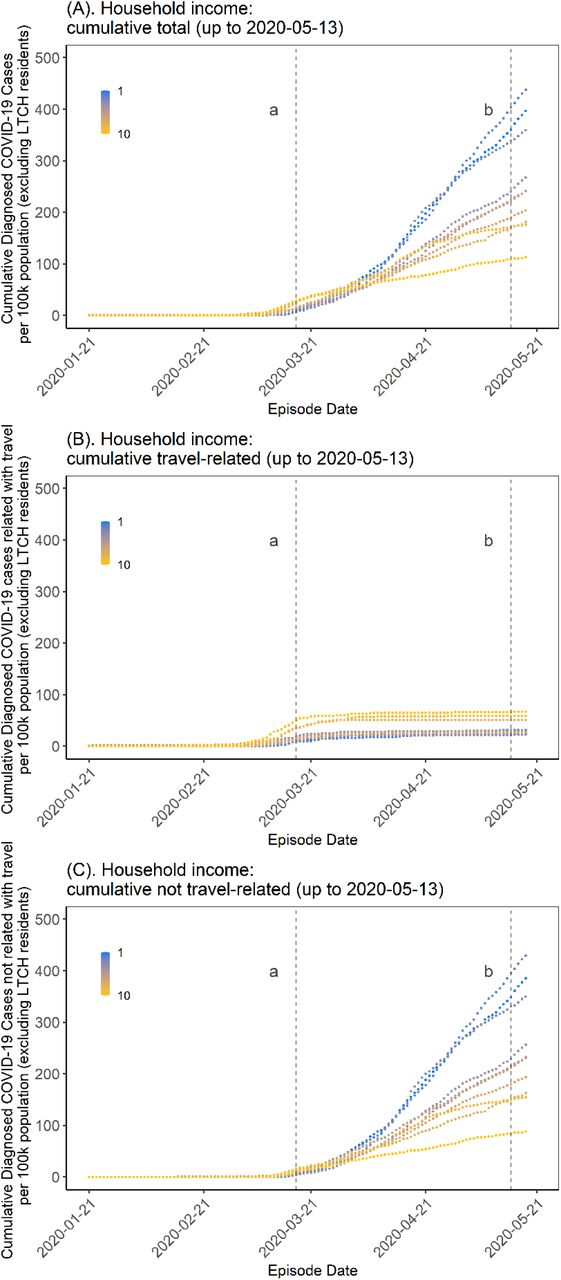
COVID-19 was initially concentrated in DAs represented by higher-income households before moving into lower-income DAs in early April 2020 (Figure 3A, Appendix Figure A4A). For the period up to May 13, 2020, travel-acquired cases were concentrated in higher-income DAs (Figure 3B). Locally acquired cases, however, although similarly concentrated in higher income neighbourhoods in the early phase of the epidemic, shifted concentration into lower income neighbourhoods (Figure 3C). A similar pattern for other social determinants was observed (Appendix Figure A5). In September, 2020, with the start of the second wave, there was a similar and consistent pattern of steeper epidemic curves among lower income neighbourhoods and slower growth in higher income neighbourhoods -a pattern replicated across the other social determinants (Appendix Figures A4B-F).

Panel A depicts all cases (excluding cases in LTCH) and demonstrates a cross-over in epidemic trajectories by DA-level income (per-person equivalent, after-tax). Early in the epidemic, per-capita rates were highest in high-income neighbourhoods but this pattern quickly reversed by early April, 2020. Panel B depicts the trajectory restricted to among travel-acquired cases which were concentrated in higher income neighbourhoods, as were the early cases before the cross-over among those not acquired through travel (Panel C). The time-periods are: (a) March 17, 2020, start of shutdown; and (b) May 14, 2020, start of stage 1 re-opening. DA: dissemination area; LTCH: long-term care homes
Concentration of cases by social determinants
The Lorenz curves and Gini coefficients of cumulative cases for the whole study period are shown in Figures 2B, 2D, and 2F; Appendix Figures A3B, A3D, and A3F, and summarized in Table 1. The largest Gini coefficients were estimated for essential workers (Gini coefficient 0.28, 95% CI: 0.23-0.34).
Mirroring to the trajectory of epidemic curves by income (Figure 2A, Appendix Figure A4A), the Lorenz curve (Figure 4) shifted over time from below to above the line of equality. The remainder of the Lorenz curves over time are shown in Appendix Figures A5A-E), and the Gini over time is summarized in Appendix Figure A6. For example, the Lorenz curve for income remained below the line of equality in the early period prior the March 16 stay-at-home order (Gini 0.25, 95% CI: 0.20-0.35) when diagnosed infections were disproportionately concentrated in higher income neighbourhoods and then consistently above the line of equality thereafter when cases were disproportionately concentrated in lower income neighbourhoods.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
The dashed line is the line of equality. The coloured solid lines represent the time periods associated with the stages of intervention: prior to shutdown (January 21, 2020 to March 16, 2020); during shutdown (March 17, 2020 to May 13, 2020); stage 1 re-opening (May 14, 2020 to June 23, 2020); stage 2 re-opening (June 24, 2020 to July 30, 2020); stage 3 re-opening (July 31, 2020 to October 9, 2020); and modified stage 2 re-opening (October 10, 2020 to November 21, 2020). Income values described are per-person equivalent and after-tax. The number of cases were initially disproportionately lower in neighbourhoods of lower income (light pink) before quickly concentrating in higher income neighbourhoods. There was less heterogeneity at the beginning of the second wave in Stage 3 (dark blue), but the epidemic concentrated again quickly by neighbourhood level income by the modified stage 2 (dark pink).
Within each time-period from the first stay-at-home order in March, the magnitude of concentration remained relatively stable during the stay-at-home orders and during Stage 1 (May-June) and Stage 2 (July-August) re-openings (Appendix Figure A6). However, when the second wave began in September, there was less heterogeneity across all social determinants (Appendix Figure A6). The Gini coefficient for income, for example, fell to 0.14 (95% CI: 0.10-0.21) before rapidly concentrating again and increasing to 0.21 (95% CI: 0.13-0.30) by the time modified restrictions resumed in October.
DISCUSSION
Using metrics of social determinants of health, we quantified increasing inequities in COVID-19 cases over time in Toronto, Canada. We found that there has been a consistent pattern, established early, of rapid concentration of COVID-19 in small geographic areas. Areas of Toronto particularly burdened by COVID-19 have lower income, dwellings characterized by household crowding, and occupations that are not amenable to remote work.
The pattern of early travel-related cases largely concentrated in higher-income and less diverse communities with fewer essential workers are similar to that observed across the globe.(2, 15, 36-38) We also found that the early, non-travel related cases were in similar neighbourhoods (i.e., higher income) suggesting a partially assortative (“like mixes with like”) physical network with respect to income-level and other social determinants. This pattern by income suggests that early, non-travel cases initially spread within higher-income networks before entering and spreading in networks represented by lower-income households. There has been limited study of population-level mixing (or “who has contact with whom”) by income and other social determinants in the context of acute respiratory infections. For sexually transmitted infections, network assortativity has been well established within sexual networks. (39) Network assortativity for COVID-19 may be driven by the overlap between social networks and transmission networks defined by greater shared airspace and opportunities for transmission where people live and work. This finding is consistent with data on social networks suggesting variable degrees of assortativity,(40) with connections between social networks through occupation-such as caregivers.(41, 42)
The observed pattern of rapid and then persistent concentration of COVID-19 by social determinants, such as household density for example, has been consistent across high-income countries(43, 44) and in several low-and middle-income countries as well.(3, 4) Where reported, occupations not amenable to remote work have also been identified as an important risk factor for COVID-19.(15) In our study setting, essential services workers intersected with multi-generational households suggesting a connection between workplace exposures and those in home communities amplified by high rates of transmission within larger households.(45)
These results should be considered in the light of limitations. We relied on area-based measures of the social determinants of health and thus our findings may be subject to ecological fallacy. There are two reassuring elements supporting validity of these findings including the use of the smallest geographical area available (DA) and the congruence of these results with individual data characterizing race and income among people with COVID-19.(46) We were also limited to broad categories with respect to occupation, and thus cannot infer concentration of cases by specific occupational exposures. Finally, these metrics for concentration or inequities are descriptive and do not independently specify a causal mechanism.
The magnitude and direction of concentration remained relatively stable after March; that is, the Gini coefficient changed little within each intervention period. The sustained inequities are consistent with data from the United States,(47) and recently reported in Toronto,(48) which suggest that mobility-based interventions-such as wide-scale restrictions-are least likely to reduce mobility in lower-income neighbourhoods.(49, 50) Collectively, workplace mobility and the Lorenz curves by non-health essential workers suggest mobility-based interventions which restrict movement may have reached saturation of impact for a subset of the population, well before the second wave in Toronto. That is, public health measures that intend to keep people at home (e.g., lockdown or stay at home orders) may have worked on only a subset of the population and potentially reinforced disparities in COVID-19 among those who could not work remotely – especially in the absence of workplace-specific occupational health interventions.
There are several implications of the findings for public health. First, findings could be used to adapt interventions and allocate resources where transmission occurs, geographically and temporally. An example of this is vaccine allocation based on per-capita risks and not just population size: i.e. the combination of geography (hence, social determinants) and age when considering vaccination priorities to allow for the joint probability of acquisition risk and severity risk when allocating limited vaccination supply in the short-term.(51) Such efforts would also need to include active, community-tailored efforts to address vaccine confidence/trust which may be lower in communities most affected by COVID-19;(52) and account for implementation challenges with neighbourhood-specific vaccine delivery ensuring it is equitable.(53, 54) Second, the occupational and housing risks identified here may be overcome with structural interventions such as paid leave, housing supports, and alleviating barriers to testing and healthcare access. While structural interventions are often considered using a long-term horizon, immediate-term activities that are implemented at scale to those who are most at risk of acquisition and transmission are feasible and are being implemented in some settings – as evidenced by community-tailored mobile testing programs and isolation support.(55, 56) These immediate actions continue to challenge the assumption that tackling social determinants can only be addressed in the long-term while passive restrictions to reduce mobility are considered feasible by decision-makers.(57, 58) For example, immediate and actionable measures to control the spread of an infectious disease can still include active, on-the-ground support for infection prevention and control in workplaces and systematically removing barriers to sick leave to support safe, voluntary, and sustainable isolation.(57, 59) Finally, public health agencies and governments can be called upon to actively measure inequities in their COVID-19 response to better understand who their interventions are reaching and who they may be leaving behind.(60)
CONCLUSIONS
In sum, there was a rapid epidemiologic transition in COVID-19 from an epidemic concentrated among higher income communities in Toronto related to travel to local transmission in lower income communities secondary to structural risks including structural racism often defining where people work and how they live. Similar to other infectious diseases the findings of marked inequities in COVID-19 burden in Toronto presented here suggests the existence of core-groups concentrated by social determinants of health. Specifically, these data characterized ‘core-groups’ that may be spatially-distributed, but whose underlying social determinants of health define the fundamental sources of heterogeneity in risks. Taken together, these findings suggest the added benefit of resource-based interventions to better address the specific needs of higher risk communities and thus reducing inequities in outcomes as has been advocated for by the local public health agencies.(61) Moreover, the inequities in the burden of COVID-19 appear to be sustained in the context of non-adaptive population-wide intervention strategies potentially secondary to the differential impact in reducing contact rates based on household density and occupation. Taken together, these results from Toronto suggest the potential impact of an equity-lens to inform resource-based policies and programs to optimize both the equity and effectiveness of COVID-19 intervention strategies.
Data Availability
Reported COVID-19 cases are not publicly available and were obtained from the Public Health Ontario Integrated Public Health Information System (iPHIS) via the Ontario COVID-19 Modelling Consensus Table and with approval from the University of Toronto Health Sciences Research Ethics Board (protocol no. 39253). A subset of iPHIS data (laboratory-confirmed cases only) were made available by the Ontario Ministry of Health and Long-Term Care (MOHLTC) to the Ontario Modelling Consensus Table on a daily basis. Variables for social determinants of health are available publicly through the 2016 Canadian Census with the exception of multi-generational households and after tax income per single person equivalent (ATIPPE). Multi-generational households data is not publicly available. ATIPPE data is available through StatsCan via the Data Liberation Initiative at academic institutions.
https://www150.statcan.gc.ca/n1/en/catalogue/98-401-X2016044.
FUNDING
This work was supported by the Canadian Institutes of Health Research (grant no. VR5-172683).
CONFLICTS OF INTEREST TO DECLARE
None
ACKNOWLEDGEMENTS
Reported COVID-19 cases were obtained from the Public Health Ontario Integrated Public Health Information System (iPHIS) via the Ontario COVID-19 Modelling Consensus Table and with approval from the University of Toronto Health Sciences Research Ethics Board (protocol no. 39253). A subset of iPHIS data (laboratory-confirmed cases only) were made available by the Ontario Ministry of Health and Long-Term Care (MOHLTC) to the Ontario Modelling Consensus Table on a daily basis. The analyses, conclusions, opinions and statements expressed herein are solely those of the authors and do not reflect those of the funding or data sources; no endorsement is intended or should be inferred.
SM is supported by a Tier 2 Canada Research Chair in Mathematical Modeling and Program Science. MM-G is supported by a Tier 2 Canada Research Chair in Population Health Modeling. SS is supported by a Tier 1 Canada Research Chair in Knowledge Translation and Quality of Care.
REFERENCES
References (continuation from main text)
- 27.




