
Abstract
Background Clinical trials on the different vaccines to SARS-CoV-2 have demonstrated protection efficacy, but it is urgent to assess the levels of protection generated with real-world data, especially in individuals professionally exposed. Measuring T-cell responses may complement antibody tests currently in use as correlates of protection but there are not validated T cell response applicable to large number of samples.
Objective To assess the feasibility of using T-cell responses to SARS-CoV-2 S peptides by commercially available whole blood interferon-gamma release assays (IGRA) as a correlate of protection.
Patients Twenty health care workers before and after vaccination.
Methods Antibody test to SARS-CoV-2 N and S proteins in parallel with one IGRA assay and two detection techniques than can be automated.
Results IGRA test detected T-cell responses in naturally exposed and vaccinated HCW already after first vaccination dose. the correlation by the two detection methods, CLIA and ELISA, very high (R>0.9) and sensitivity and specificity ranged between 100 and 86% and 100-73% respectively. Even though there was a very high concordance between antibody and the IGRA assay in the ability to detect immune response to SARS-CoV-2 there was a relatively low quantitative correlation. In the small group primed by natural infection, one vaccine dose was sufficient to reach immune response plateau. IGRA was positive in one Ig (S) antibody negative vaccinated immunosuppressed HCW illustrating another advantage of the IGRA test.
Conclusion Whole blood IGRA tests amenable to automation, as the one here reported, constitute a promising additional tool for measuring the state of the immune response to SARS-CoV-2; they are applicable to large number of samples and may become valuable correlates of protection to COVID-19, particularly for vulnerable groups at risk of being re-exposed to infection, as are health care workers.
Clinical Implications Commercial kits of whole blood Interferon-gamma release assay (IGRA) constitute an reliable method for clinical laboratories to assess T-cell response after natural infection by SARS-CoV-2 and after BNT162b2 mRNA vaccination and are suitable for large scale application.
Key Messages
Commercial kits of whole blood interferon-gamma release assay (IGRA) are potentially very useful tools to measure the T cell response to SARS-CoV-2 after COVID-19 and after SARS-CoV-2 vaccination.
One vaccine dose restores T cell response in COVID recovered patients, but the vaccination boost was required for naïve participants to attain a comparable response.
T cell response seem to decay in COVID recovered subjects after the boost second vaccination dose.
Capsule Summary Measuring T cell responses by commercially available whole blood interferon gamma release assays (IGRA) provide a promising additional correlate of protection to COVID and may be useful to reassure vulnerable group professionals at risk of being exposed to SARS-CoV-2 infection.
Introduction
One of the groups with the highest incidence of COVID-19 in the present pandemic has been Health Care Workers (HCW). In the last month of 2020 worldwide vaccination campaign to SARS-CoV-2 began and, in most countries, front line HCWs have been among the first group receiving the new vaccines. SARS-CoV-2 infection produces detectable immune responses in most cases. As part of the adaptive response to infection, humans generate SARS-CoV-2-specific antibodies and specific T lymphocytes (1). Several studies on acute and convalescent COVID-19 patients have demonstrated that SARS-CoV-2-specific T cell responses control viral replication and reduce disease severity (2). Anti-spike (S) and anti-nucleocapsid (N) proteins IgG antibodies are associated to greatly reduced risk of SARS-CoV-2 reinfection in the 6 months after COVID-19(3).
S-antigen mRNA-based vaccines against SARS-CoV2 (Pfizer-BioNTech and Moderna) have demonstrated immunogenicity (typically evaluated by serology) with 95% efficacy in more than 2 million HCW without major safety issues in all phases of human trials (4). Although clinical trial data of vaccines in use are excellent in terms of effectiveness, real-world evidence remains scarce. In particular, no papers have been published evaluating the development of T cell responses after vaccination using commercial kits suitable for large scale application. One issue arisen in the health system -as in other essential sectors- is how to reassure HCWs, especially those pertaining to vulnerable groups e.g., diabetics, that, after overcoming COVID-19 or vaccination, they are reasonably protected and can reassume their duties.
Here we present a pilot study of SARS-CoV-2 specific antibody and T responses to Spike protein (S) after mRNA vaccination in a small group of health care workers (HCWs) at Hospital Universitari Vall d’Hebron, Barcelona, Spain (HUVH) using one commercially available test suitable for clinical laboratories, amenable to automation and therefore applicable to large number of samples.
Material and Methods
Patients
Twenty HCWs on follow-up since May 2020 were recruited as part of a longitudinal study of seroprevalence and clinical impact of COVID-19 HUVH, a major academic hospital with over 6500 staff. All participants were tested before first dose (median 4 days, IQR 3), after first dose (median 22 days, IQR 1) and after the second dose (median 13 days, IQR 0) of the BNT162b2 mRNA COVID-19 vaccine (Pfizer-BioNTech, Mainz, Germany). Demographic, epidemiological, and clinical data were collected using a standard questionnaire (supplementary table 1). Five had been diagnosed of COVID-19, (COVID group) based on clinical symptoms and PCR and 15 remained unaffected (NO-COVID group).
This project was approved by the Valle de Hebron Hospital Institutional Clinical Ethical Board of HUVH (PR(AG)113/2021).
Methods
Antibody responses were measured in the clinical microbiology laboratory using two widely applied commercial CLIA assays; antibodies (IgG, IgM and IgA) to nucleocapsid (N) SARS-CoV-2 protein were detected by the qualitative Elecsys® Anti-SARS-CoV-2 test in a Cobas 8800 system autoanalyzer (both from Roche); IgG antibodies to the Spike protein were measured by the quantitative LIAISON® SARS-CoV-2 S1/S2 IgG test in a XL Analyzer (DiaSorin, Cypress, CA, USA). Samples with antibody levels >800 were diluted according to the manufacturer’s instructions. SARS-CoV-2-specific T cell responses were assessed in the clinical immunology laboratory by a whole blood Interferon-Gamma Release immuno Assay (IGRA) that uses two Qiagen proprietary mixes of SARS-CoV-2 S protein (Ag.1 and Ag.2) selected to activate both CD4 and CD8 T cells, following manufacturer’s instructions. Briefly venous blood samples were collected directly into the Quantiferon® tubes containing Spike peptides as well as positive and negative controls. Whole blood was incubated at 37°C for 16-24 hours and centrifuged to separate plasma. IFN-γ (IU/ml) was measured in these plasma samples in parallel using CLIA (Liason, Quantiferon® Gold Plus) and ELISA (QuantiFERON Human IFN-γ SARS-CoV-2, Qiagen) tests, both for research only use. Complete blood Count (CBC), flow cytometry lymphocyte phenotype and immunoglobulin levels were obtained in parallel samples (5,6).
Statistical analysis
Data were analyzed by non-parametric tests; Mann-Whitney test for comparisons between the COVID and NO-COVID groups, and Friedman test for comparisons between paired values, and correlation studies to compare variables was calculated by Pearson correlation coefficient. GraphPad Prism v8.01 software was used for both statistical analysis and graphical representation.
Results
In the COVID group plateau IgG (S) antibody levels were attained with first vaccination dose
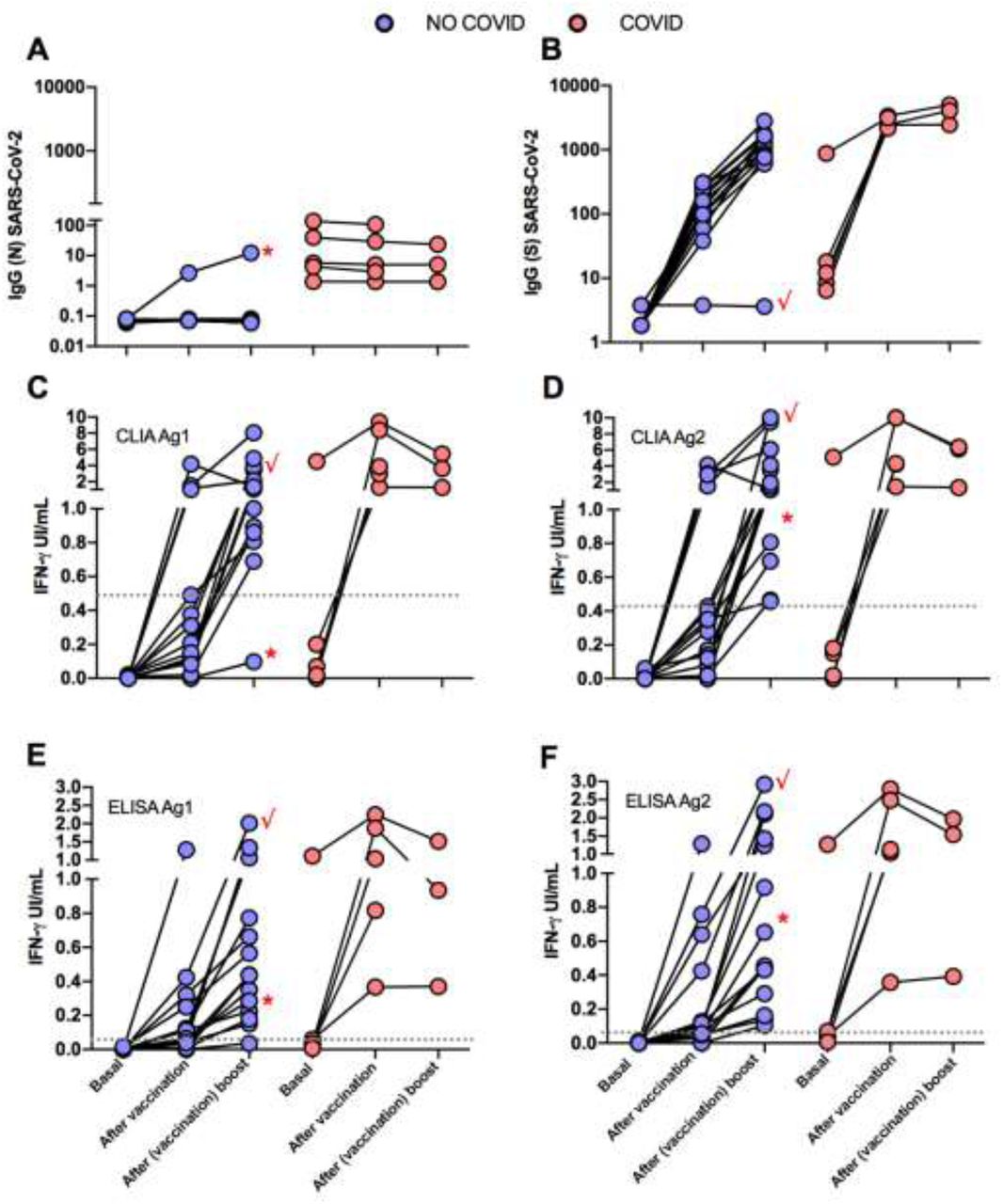
At enrolment COVID Group participants (n=5) had detectable IgG (N) antibodies while those in the NO-COVID Group, (n=15) were all negative, thus excluding the presence of asymptomatic cases in the latter group (Figure 1A). IgG(S) antibodies were measured at three time points: prior and after the vaccine first dose and after the boost second dose. NO-COVID Group participants were all negative for IgG(S) antibodies. After first vaccination, all NO-COVID subjects but one, developed IgG(S) antibodies although not reaching average levels to those found in the COVID group prior to vaccination (Mean (STDV) 150.3 (99.8) vs 2712 (511) respectively). The boost vaccine dose induced in them a further increase in IgG(S) antibody levels but not in the COVID group (Figure 1B) as if they had reached their plateau (see also Figure 2).

Antibody and cellular immune responses to SARS-CoV-2 in the two groups of HCW, NO-COVID (pink) and COVID (blue) after BNT162b2 mRNA COVID-19 vaccination at three time points: before 1st dose, before 2nd dose and after 2nd dose. A and B, results of IgG antibody levels to N (A) and S SARS-CoV-2 (B) proteins. C to F. T-cell responses to SARS-CoV-2 S peptides in two IGRA tests that measure IFN-gamma production by CLIA (A & B) and ELISA (E & F). Significance of the differences, *p<0.05, **p<0.01, ***p<0.001, ****p<0.0001.

Follow up of antibody and cellular immune responses to SARS-CoV-2 in the two groups of HCW, NO-COVID (pink) and COVID (blue) after BNT162b2 mRNA COVID-19 vaccination at three time points: before 1st dose, before 2nd dose and after 2nd dose. A and B, results of IgG antibody levels to N (A) and S SARS-CoV-2 (B) proteins. C to F. T-cell responses to SARS-CoV-2 S peptides in two IGRA tests that measure IFN-gamma production by CLIA (A & B) and ELISA (E & F). Patient 12 (√) and patient 19 (*) are labelled by red symbols.
IGRA detects specific cellular response to SARS-CoV-2 with high sensitivity and specificity using either CLIA or ELISA tests to measure IFN-gamma production
Results from IFN-gamma production to Ag.1 and Ag.2 S peptides measured by CLIA are in Figure 1C and D and by ELISA in E and F. The correlation of CLIA and ELISA readings was almost total (R>0.9) in all cases.
Cut-off points for each variant of the IGRA assay were calculated by ROC analysis with the following results: CLIA cut-off point was > 0.051 IU IFN-gamma/ml with a sensitivity of 86% and specificity of 100% for Ag1 and > 0.442 for Ag2 with a sensitivity 100% and a specificity 73% (Supplementary Figure 1). The cut-off point for the ELISA was >0.0065 IU IFN-gamma/ml for Ag1 with a sensitivity of 86.67% and specificity 92% and for Ag 2 > 0.024 with a sensitivity of 80% and a specificity of 100%. Correlation between Ag1 and Ag2 results was very high (R=0.9 for ELISA and 0.8 for CLIA (data not shown). In general Ag.2 induced higher responses than Ag.1, and. A positive response to either of the two peptides pools should be considered, in principle a positive result. From these results it is not clear the need of using the Ag. 1 pool of peptides but this may be different in a larger group with a more diverse genetic background.
Overall quantitative correlation between the antibody and T cell responses was low (R in the order of 0.2) (Supplementary figure 2) but there was a good concordance in detecting the immune response to Spike. Sensitivity of the IGRA test may be superior in this group to IgG(S) antibody test due to the presence of one anti-CD20 treated participant (see below, illustrative case 12), but due to the small size, conclusions cannot be drawn.
One vaccine dose restores T cell response in post COVID participants, but vaccination boost was required for naïve participants to attain a good response
Interestingly four of the five post COVID participants did not respond in the IGRA test prior to vaccination, but one dose was sufficient to reach good levels of IFN-gamma production, indicating priming by the natural infection. Second dose rather reduced the response, perhaps because due to the time elapsed since priming, response contracted more quickly, this reduction has now been reported in two not yet peer reviewed reports (7 ,8). In the NO-COVID group even if the first dose already induced a significant response, the boost vaccination was required to reach a response similar to that of the COVID after first dose.
In this small study we did not find any relation of antibody nor T cell responses to Spike proteins with the total lymphocytes, their main subsets or the immunoglobulin levels. There was a trend of responses of antibody and T-cell responses to be lower in older patients (Supplementary figure 3), no gender effect was detected.
Illustrative HCW cases
As mentioned above one of the NO-COVID patients, case 12, was treated with anti-CD20 for an autoimmune condition and did not develop IgG or IgM antibodies after vaccination. Interestingly a clearly measurable T-cell responses was detected (see Figure 2 tick case) after vaccination and a small expansion of circulating of plasmablasts in sequential samples. We detect plasmablast after the vaccine boost with few pre class switch B lymphocytes prior to vaccination despite anti-CD20 treatment, indicating residual capacity of the B cell compartment (Supplementary figure 4).
Another NO-COVID group patient, case 19, was infected the same day that received first dose of vaccination. The patient developed T cell response in the IGRA assay, and in this case, in addition to antibodies to the S antigen, she developed antibodies to N antigen (Figure 1 A, dot with asterisk), but the response was like the NO-COVID group indicating that being primed by two simultaneous stimuli did not result in this case in a supranormal response.
Discussion
We have studied in parallel antibody and cellular response to the BNT162b2 mRNA COVID-19 vaccine in a small group of HCW and found that the IGRA assays yields rapid results that are concordant with antibody tests and could constitute a valuable contribution to the evaluation on the immune response in people that may need to be reassured of being protected to SARS-CoV2 infection. This is however a pilot small study that should be expanded to really demonstrate that SARS-CoV-2 Spike IGRA based tests can constitute valuable correlates of protection complementary to serology.
It has already been shown that protein N is the most immunogenic structural protein and that IgG responses to protein S in SARS-CoV-2 are lower, possibly due to the glycosylation state of this protein (9). This may explain that IGRA and IgG(S) antibody tests were negative in two of the participants in the COVID group that were IgG (N) positive. However, after immunization with a single dose, they responded to a level higher than fully vaccinate no COVID participants.
There are a good number of studies demonstrating T cell responses to SARS-CoV-2 using technique widely applied to measure responses to other viral infection (10,11). These techniques include intracellular cytokine staining (ICS) by flow cytometry and variations of the ELISPOT assay which measure mainly IFN-gamma production. Activation-induced markers (AIM), also by flow cytometry, can be a sensitive technique (12). However, they have limitations in the applicability compared with whole IGRA blood assays used here when it comes to use them in a clinical laboratory (13).
Availability of a complementary correlate of protection in addition to serology may be invaluable for to two groups, 1) HCW and other professionals with vulnerability factors that need to be reassured of being immunized to SARS-CoV2 before reassuming tasks that have a risk of accidental re-exposure and 2) for immunosuppressed patients that fail to make a measurable antibody response. IGRA Spike peptides test may constitute a very valuable tool in this context as can be applied to a large number of samples producing results in 24h and with promising sensitivity and specificity.
Data Availability
27-March-2021
Author disclosure statement
The authors declare that they have no conflict of interest. All the authors have read and approved the text submitted.
V.S.M. I.A.M. and C.F.N. participated in performing the research and data analysis.
R.P.B., V.C., A.A.P., M.H.G. and T.M.S participate in critical review of the manuscript.
M.M.G. J.E.E. and M.L.H. participated in conducting the study, writing and reviewing the manuscript.

Analysis of the methods for assessing cell-mediated immunity by SARS-CoV-2 IGRA-type CLIA (A and B) and ELISA (C and D) using ROC curves comparing basal and after vaccine study points in NO-COVID group.

Correlation between the antibody and T cell responses with different IFN-g detection methods ELISA (A and C) and CLIA (B and D). Correlation between the T cell response to Ag1 and Ag2 with ELISA (E) and CLIA (F).

Correlation between age and T cell responses with different IFN-g detection methods ELISA (A, C, E and G) and CLIA (B, D, F and H) with Ag1 and Ag2; after vaccine (A,B,C and D) and after (vaccine) boost (E,F,G and H).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Analysis of naive B lymphocyte subpopulations in patient 12. Class switch, IgM memory and plasmablasts before vaccination (A), after first dose (B) and second vaccination dose (C) Memory/switch B lymphocytes were already present before vaccination and plasmablasts appeared only after vaccination.
ACKNOWLEDGEMENTS
The authors want to express their gratitude to participants of the study and laboratory technicians from Microbiology and Immunology for technical assistance. We thank Qiagen and Diasorin for commercial kits donation, these companies do not participate in the experimental plan, data analysis nor in writing this manuscript. English writing support was provided by Fidelma Greaves.
This study was funded in part by Instituto de Salud Carlos III, grant COV20/00416 co-financed by the European Regional Development Fund (ERDF).
Abbreviations
- (HCWs)
- Health care workers
- (IGRA)
- Interferon-gamma release assays
- (CLIA)
- Chemiluminescence immunoassays
- (ELISA)
- Enzyme linked immunosorbent assay
- (CBC)
- Complete blood count
- (S)
- Spike protein
- (N)
- Nucleocapsid protein




