
Abstract
Objective Uptake for cervical cancer screening remains well below the recommended rate of 80%. We conducted a pilot study to determine the reasons for non-attendance and explore their acceptance of human papillomavirus (HPV) self-sampling as an alternative to Pap test.
Methods A two-part cross-sectional study was conducted at a health centre in Brunei, from January to December 2019. Women who were eligible for a Pap test but who either never or did not have one within the past four years were conveniently recruited. Participants were first asked to complete a paper-based survey on their reasons for screening non-attendance, and then invited for HPV self-sampling. Results were analysed using descriptive and inferential statistics.
Result We enrolled 174 screening non-attendees, out of which 97 (55.7%) also participated in HPV self-sampling. The main reasons for not attending Pap test screening were fear of bad results (16.1%, n = 28); embarrassment (14.9%, n = 26) and lack of time due to home commitments (10.3%, n = 18). When compared to those who agreed to participate in HPV self-sampling, those who declined were significantly older (p = 0.002) and less likely to agree that they are susceptible to cervical cancer (p = 0.023). They preferred to receive Pap-test related information from healthcare workers (59.0%, n = 155), social messaging platforms (28.7%, n = 51) and social media (26.4%, n = 47). HPV self-sampling kits were positively-received, where > 90% agreed on its ease and convenience. Nine of 97 participants (9.3%) tested positive for hr-HPV, out of which eight were non-16/18 HPV genotypes.
Conclusion Our findings suggest that promoting knowledge on cervical cancer, the benefits of screening and clarifying any misconceptions of Pap test results would help increase screening uptake among Bruneian non-attendees. Response to HPV self-sampling was highly positive, implying its receptiveness in the local setting. Our high detection of non-16/18 HPV genotypes suggest high prevalence of other hr-HPV genotypes in Brunei. Larger studies can be conducted to further validate our findings.
Introduction
Cervical cancer is highly preventable but still remains one of the most common cancers among women worldwide, accounting for 6.6% of all female cancer deaths in 2018 [1]. Cervical cancer screening has drastically reduced the incidence of invasive cervical cancer in countries that have implemented such screening programmes [2], which traditionally involves the use of the standard Papanicolaou (Pap) test. However, as specific high-risk human papillomavirus subtypes (hr-HPV) are known to be a causative agent, the use of HPV self-sampling is becoming either an alternative or a complement to the Pap test to increase screening uptake rate [3], particularly to promote women’s participation among screening non-attendees [4].
HPV self-sampling were found to be highly acceptable among non-attendees [5,6]. Repeated HPV self-sampling and testing were shown to increase screening uptake [3,4,7], and also resulted in at least two-fold higher detection rate of high-grade cervical intraepithelial neoplasia (CIN2+) when compared to Pap test [8,9]. In addition, HPV self-sampling results exhibit similar sensitivity and specificity compared to results from samples taken by trained professionals [10]. At the national level, early detection through organised screening had been shown to reduce cervical cancer morbidity and mortality in countries such as the United Kingdom and Australia [11,12]. Both countries have further strengthened their national cervical cancer screening programme by replacing cytological test with HPV test as the primary screening test.
Brunei Darussalam (population 459,500) is a small Southeast Asian country with a predominant Muslim population and a crude birth rate of 15.3 per 1,000 population [13]. Within this region, it has one of the highest age-standardised incidence rate (ASR) for cervical cancer: 20.6 in Brunei when compared to 10.5 and 7.7 in Malaysia and Singapore, respectively [14]. Brunei has initiated a national cervical cancer prevention and control programme since 2009, which include setting up the National Pap Test Registry, organising cervical screening through periodic mail invitations for sexually-active women aged 20 to 65 years, replacing the conventional Pap test with liquid-based cytology, and initiating HPV vaccination for school-aged female adolescents [15]. However, despite cervical screening being offered free of charge, the national screening coverage rate remains low at 44% in 2018 (unpublished data). Non-attendees of cervical screening are at increased risk of developing cervical cancer; hence the importance of reaching these women [16]. Reasons for screening non-attendance can also vary across settings [17,18].
With Brunei’s relatively high incidence of cervical cancer and low screening uptake, we conducted a pilot study to explore the reasons behind non-attendance and assess the acceptability of HPV self-sampling as a possible alternative to the Pap test among non-attendees. Study findings could be used to strategise ways to improve screening coverage and provide preliminary evidence towards implementing HPV testing as the primary screening test for cervical cancer in Brunei.
Methods
Study design and data collection
We conducted a two-part cross-sectional survey at Jubli Perak Sengkurong Health Center (JPSHC), from January to December 2019. JPSHC is a government-funded health centre located in Brunei-Muara District, where the majority (69.3%) of the country’s population resides. This centre provides primary health care services to Mukim Sengkurong, a sub-district with about 32 000 people from various socioeconomic backgrounds.
Eligible women attending either the outpatient or child health clinic were conveniently recruited by triage nurses. The inclusion criteria were married or ever married Bruneian women between 20 and 65 years old, who never had a Pap test or did not have a Pap test within the last 4 years, and who can comprehend Brunei-Malay or English language. Women who were either pregnant, have had total hysterectomy, or with a history of malignancies were excluded.
Following recruitment, potential participants were referred to an assigned research focal person based at JPSHC. The participants were informed of the study objectives and of the two study parts; the first involving a set of self-administered questionnaires on reasons for non-attendance to routine cervical screening (Q1), and the second (optional) part involving HPV self-sampling to be performed at a later date and completing a second self-administered questionnaire on their acceptability of the self-sampling procedure (Q2).
Participants who consented to the first part of the study were asked to complete Q1 onsite. They were then given an envelope containing information on the second optional study and an instruction leaflet on the HPV self-sampling procedure. Within two weeks, they were contacted by the focal person regarding their decision to participate in the second part of the study. Those who agreed to participate were given an appointment to JPSHC. On the appointment day, a trained nurse first explained the self-sampling procedure with the aid of an online instructional video, and answered any questions or concerns. Then, participants were given a self-sampling kit and asked to perform the self-sampling procedure in the clinic. After completing the procedure, the participants were invited to complete Q2.
Questionnaires used
Two bilingual paper-based questionnaires (Brunei-Malay and English language) were used: one on the reasons for non-attendance (Q1) and another on their acceptability of the self-sampling procedure (Q2). Both questionnaires were adapted from similar studies [19,20]. They were first translated to Brunei-Malay language by native speakers, and then back-translated to check for inconsistencies in comprehension. Both questionnaires were also pre-tested on six eligible women to assess if the questions can be easily understood. Responses from pre-testing were not included in the main analysis.
Q1 consists of 19 questions on the participant’s socio-demographics; reasons for not getting Pap test; attitude and knowledge on cervical cancer; and lastly, preferred sources to acquire information about Pap test. From a prepared list of 16 options, participants were asked to select one (“Major” reason) or more reasons (categorized as “Minor” reasons) for not attending the screening programme. Responses for questions on their attitude and knowledge on cervical cancer were assessed using a five-point Likert scale, ranging from “Strongly Agree” to “Strongly Disagree”. Q2 consists of 12 five-point Likert scale questions (ranging from “Strongly Agree” to “Strongly Disagree”) on their experiences and opinions of the self-sampling kit.
Self-sample handling and laboratory testing
Swabs collected from the self-sampling kits were sent to an overseas laboratory (at BNH hospital, Thailand) for hr-HPV testing. The self-sampling device used was the Evalyn® brush from Rovers Medical Devices. Upon receipt at the testing laboratory, the dry Evalyn® brush was suspended in SurePath medium from which a sample was obtained for the identification of the presence of hr-HPV using the cobas HPV test (Roche, USA). Cobas HPV tests are automated qualitative in vitro tests for the detection of HPV DNA in patient specimens. The tests utilize amplification of target DNA by polymerase chain reaction (PCR) and nucleic acid hybridization for the detection of 14 hr-HPV types (namely genotypes 16, 18, and 12 pooled hr-HPV genotypes 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, 66 and 68) in a single analysis. Results obtained from this test can be categorized into four groups: Negative, HPV-16 positive, HPV-18 positive, and positive for non-16/18 HPV genotypes.
Clinical management of hr-HPV positive participants
We adopted the cytology triage strategy for HPV self-sampling participants [21]. Participants with hr-HPV positive results were invited for an immediate clinic-based cytology triage test. Those found to have negative cytology results were invited for a repeat cytology triage test after six months. Those with second negative results were returned to routine cervical screening recall. Participants with any positive cytology result (defined as with Atypical Squamous Cells of Undetermined Significance or worse) were referred for colposcopic examination.
Statistical analysis
Descriptive statistics was conducted to characterize the socio-demographic characteristics of the study population, their reasons for not attending screening, their attitudes and preference for information access on such screening, as well as responses from Q2. Mann-Whitney and Fisher’s exact tests were used to assess significant differences in sociodemographic characteristics between women who agreed and women declined to proceed to the HPV self-sampling part of the study. Responses for questions with the five-point Likert scale were categorized into three categories (agree, neutral, and disagree), and those with missing values were classified as neutral. Analysis was conducted using R ver. 3.6 [22]. Ethics approval was obtained from the Medical and Health Research and Ethics Committee (MHREC), Ministry of Health, Brunei Darussalam [Reference no. MHREC/MOH/2018/9(2)].
Results
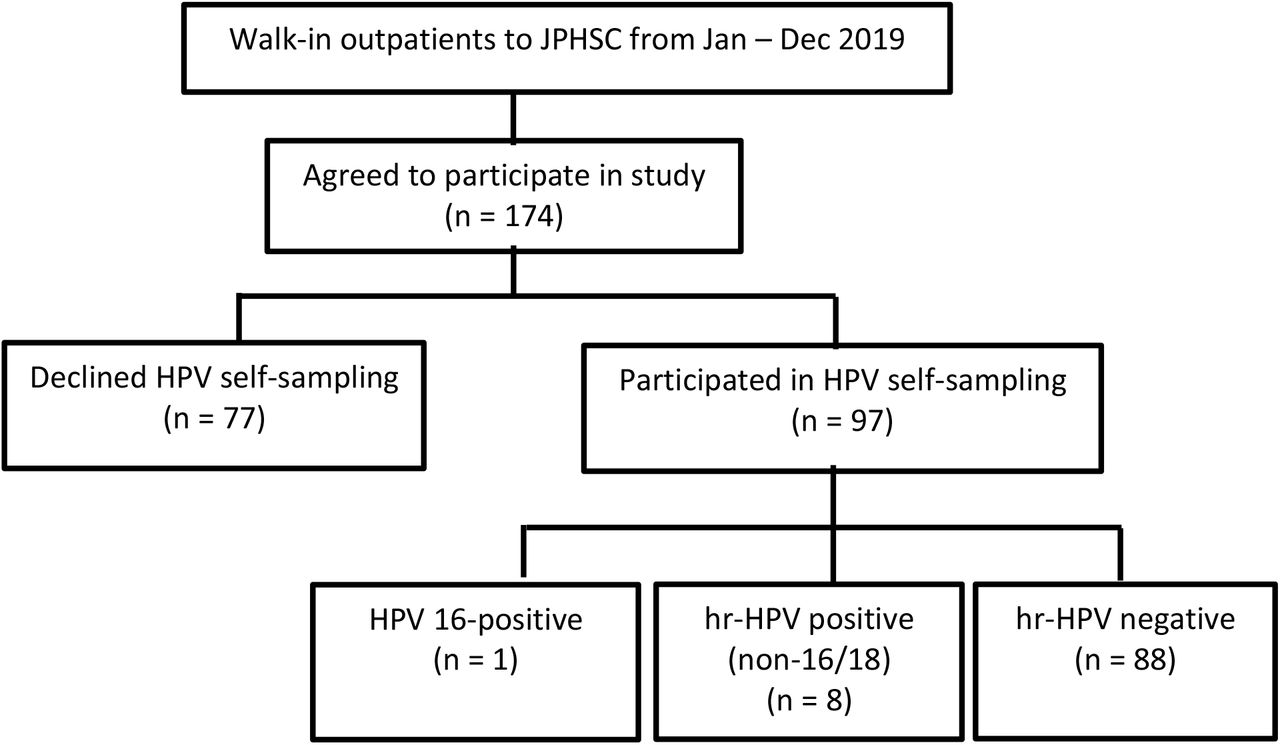
A total of 174 eligible women were enrolled into the study from January to December 2019, out of which 97 (55.7%) also participated in HPV self-sampling (Figure 1). Their median age was 45 years, ranging between 23 and 65 years (Table 1). The participants were mainly of Malay ethnicity (92.5%, n = 161), married (90.2%, n = 157), and had three or more births (60.3%, n = 105). More than half of the participants had their last Pap test performed between 4 and 10 years ago (52.3%, n = 91) and have never received the HPV vaccine (54.6%, n = 95). There were significant differences between those who agreed and declined to participate in HPV self-sampling: those who declined were significantly older (p = 0.002) and more likely to have their last Pap test performed more than 10 years ago (p = 0.031).
Sociodemographic characteristics of the study population, including comparison between groups that agreed and declined to join HPV self-sampling. IQR = Interquartile range.

Flowchart of study participants at JPHSC, Brunei (Jan – Dec 2019)
Figure 2 and Table S1 show the responses for the major and minor reasons for not attending cervical cancer screening. The top three major reasons reported were that they were “afraid of getting a bad result” (16.1%, n = 28), “feeling embarrassed being examined by a doctor or nurse” (14.9%, n = 26), and “I can’t find the time as I’m too busy at home” (10.3%, n = 18). The top three minor reasons were “feeling embarrassed being examined by a doctor or nurse” (20.7%, n = 36), “I can’t find time as I’m too busy at work” (20.7%, n = 36), and “afraid of getting a bad result” (20.1%, n = 35).

Responses on their major and minor reasons for not attending cervical cancer screening, among non-attendees at JPSHC (Jan – Dec 2019). The x-axis indicates the percentage, and the number next to each bar indicates the actual number of responses.
When comparing top 10 major reasons for not attending screening between those who agreed and declined HPV self-sampling (Table 2), those whose major reason was “feeling embarrassed being examined by a doctor or nurse” were significantly more likely to join self-sampling (p = 0.020). Also, those whose major reason was “afraid of getting a bad result” were significantly more likely to decline self-sampling (p = 0.034). Among those who were employed (n = 98), about a quarter (23.5%, n = 23) reported work-related reasons as their major reason for not attending screening (“I can’t find the time as I’m too busy at work” and “Difficult to get permission from employer”).
The top ten major reasons of not attending cervical cancer screening at JPSHC, Brunei (Jan – Dec 2019), with comparison between those who agreed and declined HPV self-sampling. Responses from 146 participants (83.9% of the total study population) were included.
While there is a variation in the responses when asked about their health and susceptibility to disease, most agreed on the benefits of undergoing Pap test (92.0%, n = 160) and on the severity of cervical cancer (82.8%, n = 144; Table 3).
Attitudes towards cervical cancer screening among non-attendees at JPSHC, Brunei (Jan – Dec 2019). Responses from the total study population (n = 174) were included.
When comparing the responses for each attitude question between those who agreed and declined to join HPV self-sampling (Table 4), those who agreed that they are more susceptible to develop cervical cancer were significantly more likely to join HPV self-sampling (p = 0.023).
Comparison of the attitudes towards cervical cancer screening among non-attendees at JPSHC, Brunei (Jan–Dec 2019), between those who agreed and declined HPV self-sampling. Responses from the total study population (n = 174) were included.
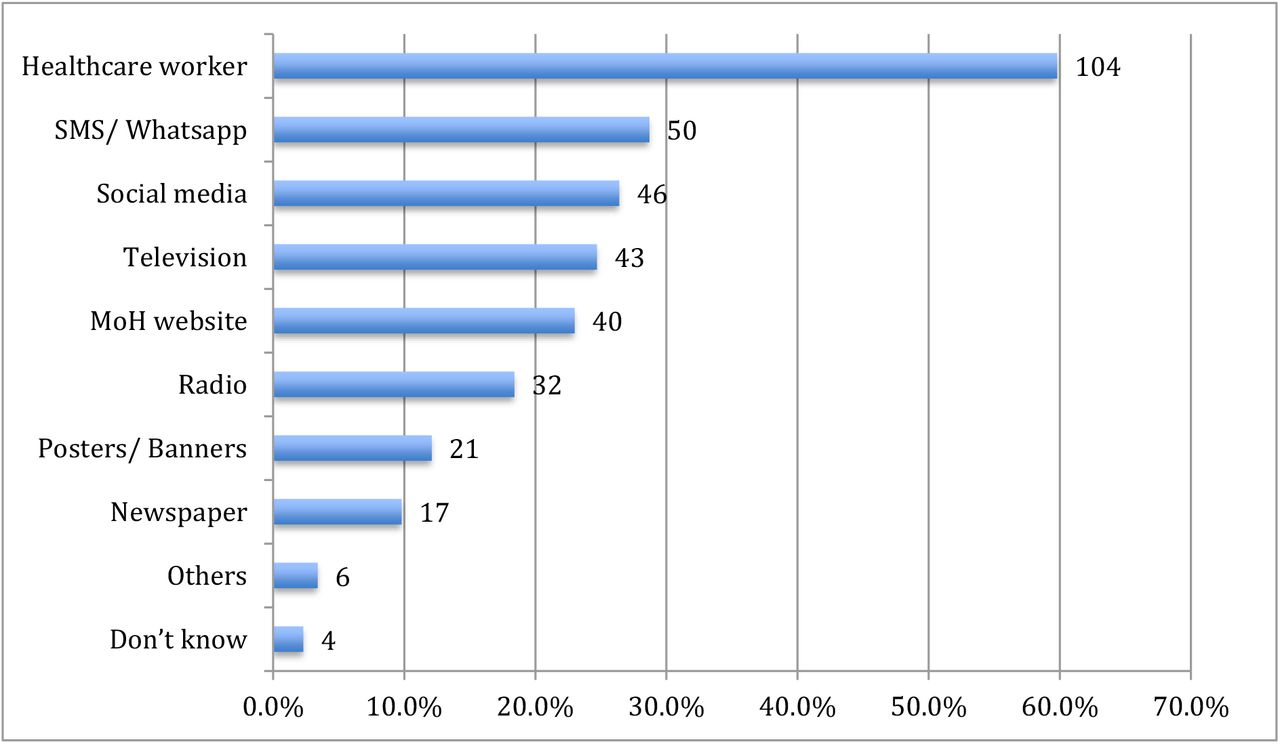
Most participants responded that they would like to obtain more information about cervical cancer screening (85.6%, n = 149). The top preferred information sources were healthcare workers (59.8%, n = 104), social messaging platforms (28.7%, n = 50) and social media (26.4%, n = 46; Figure 3).

{kind=link}
{kind=link}
{kind=link}
Preferred sources of information about cervical cancer among non-attendees at JPSHC, Brunei (Jan–Dec 2019). The x-axis indicates the percentage, and the number next to each bar indicates the number of responses. Multiple responses were allowed and responses from the total study population (n = 174) were included.
Among those who participated in self-sampling (55.7%, n = 97), their responses on the use of the self-sampling kit (Table 5) were generally positive and encouraging. A majority agreed that the instructions were clear (94.8%, n = 92), that it was easy to perform the swab (93.8%, n = 91), and that it was more convenient than the Pap test (91.7%, n = 89). They also reported their confidence in correctly getting the sample (92.8%, n = 90), would prefer to use this method next time (94.8%, n = 92), and would recommend this method to other women (93.8%, n = 91). Notably, 54.6% (n = 53) still prefer a proper Pap test for their subsequent check-up.
Acceptability of HPV self-sampling among non-attendees who participated in HPV self-sampling at JPSHC, Brunei (Jan–Dec 2019). Responses from all respondents for Q2 (n = 97) were included.
Among the 97 samples taken, nine (9.3%) tested positive for hr-HPV: one was positive for HPV 16 and eight were positive for non-HPV 16/18 HPV genotype. Upon follow-up cytology, only one participant had a normal cytological test result, whilst another participant with non-16/18 HPV genotype was found to have CIN 3 with glandular involvement following a confirmatory biopsy. No significant differences were observed when comparing the sociodemographic characteristics between those who tested hr-HPV positive and those who tested hr-negative (Table S2).
Discussion
This two-part pilot study explored the reasons for cervical screening non-attendance among Bruneian women and whether HPV self-sampling is a viable alternative for the non-attendees. Our findings highlight three important points to consider for improving both screening uptake and detection of cervical cancer.
First, our findings suggest that it is necessary to provide accurate information among Bruneian women on cervical cancer, the importance of screening and addressing any misconceptions about the Pap test. Important facts to relay include the slow development from pre-cancerous changes to cervical cancer, that pre-cancerous changes are highly treatable, and that screening will help in early detection and thus facilitate successful treatment. This is evident in our study, where emotional barriers (fear of unfavourable test results and embarrassment) were the most common major reasons of screening non-attendance. Many women have misconceptions about abnormal Pap test results by relating them to cervical cancer diagnoses [23]. It is not surprising then that almost two-thirds of the women who cited this as their main barrier declined to take part in HPV self-sampling part. As our study participants are predominantly Malays and thus of Islamic faith, religious and cultural modesty could also be a contributing factor for embarrassment among Muslim women [24].
Lack of information or knowledge has been suggested to reduce women’s concerns towards cervical cancer [25] and whether to continue attending cervical screening [26]. Although fear, embarrassment and other psychosocial barriers may play a large role at the onset of screening programme, its role diminishes over time with increasing education and knowledge of screening [27]. Educational interventions could also benefit the small group of women who cited menopause, cessation of child-bearing and having had HPV vaccination as reasons for not attending screening.
Promoting cervical cancer awareness could also impact non-attendees’ decision to participate in HPV self-sampling. In our study, we observed those who agree that they are susceptible to cervical cancer were significantly more likely to participate in HPV self-sampling. This suggests that perceived susceptibility could be an important factor for self-sampling participation, whereby those who do not perceive themselves as susceptible were less likely to engage in preventative behaviours [25,28,29]. Perceived susceptibility can be increased through education to improve their beliefs on the necessity of screening [30]. We suggest that such information could be more effectively disseminated as simple health messages endorsed by Brunei’s Ministry of Health via website, social media platforms, and the BruHealth application [31] developed by the Brunei government as a public engagement tool during the COVID-19 pandemic.
Second, we observed high acceptability of HPV self-sampling among our participants. Indeed, meta-analyses have indicated strong acceptance of self-sampling and a preference for the latter over clinician sampling [32], mainly due to logistical reasons [33]. Implementing HPV self-sampling in screening programmes have been shown to increase the screening uptake among non-attendees [3,4,7], and also increases the detection of CIN 2+ lesions [8,9]. Providing HPV self-sampling as a cervical cancer screening option could also encourage those, whose main reason for not attending was fear of pain due to previous experience, to attend screening. This reason, also common in our study, was reported as a factor for avoiding screening [34] and is suggested to predict future screening uptake [35]. Among those who joined HPV self-sampling in our study, at least half cited embarrassment, fear of pain or lack of time due to home and/or work commitments as their major reason of not attending screening. This suggest that flexibility to accommodate women’s screening method preference [36], such as the option to carry out self-sampling [37], could improve screening uptake.
Notably, only about three-quarters of our self-sampling participants were confident of the result accuracy and less than two-thirds were willing to do the self-sampling at home, suggesting that these participants could be doubting their technique and would prefer to do this in clinics instead. Also, more than half of them were willing to undergo in-clinic Pap test for their subsequent testing. This is an important consideration if cytology triaging is going to be the country’s strategy as a follow-up to HPV screening.
Thirdly, most of the detected hr-HPV genotypes in our study were non-16/18, with only one out of nine participants tested positive for HPV 16. Even though our sample size is small, this result suggests that it may not be accurate to assume HPV 16 or 18 as common hr-HPV genotypes in Brunei, although this is true in the global context [38]. Other studies have detected a significant percentage of non-16/18 hr-HPV genotypes, suggesting the presence of region-specific heterogeneity in the HPV genotype distribution [38–42]. Also, variation in HPV distribution among different ethnic groups has been reported in an American study [43], although reasons for these differences are unclear. Our finding has potential implication on Brunei’s national school-based HPV vaccination programme which currently provides vaccines which do not confer protection against non-16/18 genotypes. Providing vaccines that confers protection against nine hr-HPV genotypes [44] could be a better alternative for Bruneian females. Larger population-based studies to understand the distribution of HPV genotypes among Bruneian women will be crucial to determine the efficacy or impact of the current vaccines.
A major limitation for this study is that non-attendees from only one health center were recruited, thus our results are not representative of the adult female population in Brunei. Moreover, the validity of our findings could be compromised due to the small sample size. Our study findings, even at this pilot stage, could encourage stakeholders to conduct similar studies with larger population coverage. Also, as this study relied on the self-reported history of previous Pap test attendance, we might have missed recruiting those who may have forgotten their last Pap test date.
In conclusion, our findings indicate the need to further promote education and awareness towards cervical cancer and its screening process. Reasons of cervical cancer screening non-attendance were mainly related to emotional and logistical factors. As we found high acceptance towards HPV self-sampling, this could be adopted as an alternative for women who refrain from Pap test. Our high detection of non-16/18 HPV genotypes suggest high prevalence of other hr-HPV genotypes in Brunei. Future larger studies involving more Bruneian women can be done to verify our results. Follow-up studies should also be done to consider HPV testing as the suitable method for cervical cancer screening.
Data Availability
Dataset used for this study can be obtained from the corresponding author, upon reasonable request.
Funding
Funding for this study was obtained from the Ministry of Health, Brunei Darussalam.
Author contributions
Liling Chaw: Conceptualization, Methodology, Data curation, Formal analysis, Supervision, Writing - original draft, Writing - review & editing
Shirley HF Lee: Visualization, Writing - original draft, Writing - review & editing
Nurul Iffah Hazwani Ja’afar: Investigation, Data curation, Writing - original draft
Edwin Lim: Conceptualization, Methodology, Resources, Funding acquisition, Supervision, Writing - review & editing
Roslin Sharbawi: Conceptualization, Methodology, Resources, Funding acquisition, Investigation, Project administration, Supervision, Writing - original draft, Writing - review & editing
Supplementary information
Responses on their major and minor reasons for not attending cervical cancer screening among non-attendees at JPSHC, Brunei (Jan – Dec 2019)
Socio demographic characteristics and comparison between screening non-attendees who tested positive and negative for hr-HPV at JPSHC, Brunei (Jan – Dec 2019),
Acknowledgements
The authors would like to thank the JPSHC staff who have assisted in participant recruitment and questionnaire distribution.
References




