
Summary
Background Although the number of COVID-19 (coronavirus disease 2019) cases continues to increase globally, there are few studies on the clinical characteristics of children and adolescents with COVID-19.
Objective To conduct a comprehensive systematic evaluation and meta-analysis of the clinical characteristics of COVID-19 in children and adolescents to better guide the response to the current epidemic.
Methods We searched PubMed, Embase, the Cochrane Library, Web of Science, CNKI (Chinese database), Clinical Trials.gov and chictr.org.cn (China). The methodological quality of the included literature was evaluated using the Quality Assessment Tool for Case Series Studies. Meta-analysis was performed using STATA 14.0. Heterogeneity was assessed by the Q statistic and quantified using I2. We used fixed-effects or random-effects models to pool clinical data in the meta-analysis. Publication bias was evaluated by the Begg’s test.
Results We analyzed 49 studies involving 1627 patients. In the pooled data, the most common clinical symptoms were fever (56% [0.50−0.61]) and cough (45% [0.39−0.51]). The most common laboratory abnormalities were elevated procalcitonin (40% [0.23−0.57]), elevated lactate dehydrogenase (31% [0.19−0.43]), increased lymphocyte count (28% [0.17−0.42]), increased creatine kinase (28% [0.18− 0.40]), and elevated C-reactive protein (26% [0.17−0.36]). The most common abnormalities determined by computed tomography were lower-lobe involvement (56% [0.42-0.70]), ground-glass opacities (33% [0.25−0.42]), bilateral pneumonia (32% [0.24-0.40]), patchy shadowing (31% [0.18-0.45]), and upper lobe involvement (30% [0.20-0.41]).
Conclusion Disease severity among children and adolescents with COVID-19 was milder than that among adult patients, with a greater proportion of mild and asymptomatic cases, and thus, the diagnosis of COVID-19 and control of the infection source are more challenging.
Introduction
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) is a newly discovered coronavirus responsible for the coronavirus disease 2019 (COVID-19), which was first reported in Wuhan City, Hubei Province in December 2019 [1]. On January 12, 2020, the World Health Organization (WHO) officially named the novel coronavirus “2019 novel coronavirus (2019-nCoV)” [2]. So far, over 20□million people live with COVID-19 worldwide, with 750,000 deaths, and the death toll is still rising. Currently, COVID-19 outbreaks are continuing to spread across the globe. SARS-CoV-2 is spread by between-human transmission via droplets or close contact [3], but there are also studies showing that it can be transmitted from person to person by aerosols [4]. Fecal-oral routes may also constitute a potential person-to-person transmission route. Several studies have reported that the virus may still be transmitted from COVID-19-positive stool samples even after COVID-19 with negative detection of viral ribonucleic acid from nasopharyngeal swabs [5,13]. The development of the immune system in children and adolescents is not yet perfect, and it is easy for various types of viruses to cause infections. COVID-19 is a novel infectious disease. The population lacks immunity and is generally susceptible in crowded conditions. However, a study has found that COVID-19 in children below the age of 10 years constituted only 0.35% of cases [6].It is essential to identify and control patients who are suspected of having COVID-19 as early as possible and to prevent the further spread of the epidemic by controlling the source of infection and cutting off transmission pathways. Although the number of COVID-19 cases continues to grow globally, there are few studies focusing on the clinical manifestations, laboratory tests, chest imaging examinations, and complications for children and adolescents with COVID-19. We conducted a systematic review and meta-analysis of the clinical characteristics of children and adolescents to describe comprehensive characteristics of COVID-19 in children and adolescents to better treat and control the current outbreak.
1 Methods
1.1 Retrieval of published studies
PRISMA and MOOSE guidelines were used to conduct this systematic review and meta-analysis [7–8]. We used the Medical Subject Heading (MeSH) terms and corresponding keywords to develop the search strategy. The search terms included: “Child (MeSH)” or “children” or “Adolescent (MeSH)” or “Teens” and “COVID-19 (MeSH)” or “SARS-CoV-2 infection” and “clinical characteristics” or “clinical features”. We searched PubMed, Embase, the Cochrane Library, Web of Science, and CNKI (Chinese database). We also searched Clinical Trials.gov and chictr.org.cn (China) to find unpublished studies. There were no restrictions on use, including no language restrictions. The search time limit was from the establishment of each database to July 10, 2020. To ensure comprehensiveness of the search strategy, the search tasks were performed independently by two researchers (LL, BT). Details of the search strategy are provided as shown in Supplementary Text S1.
1.2 Inclusion and exclusion criteria
1.2.1 Inclusion criteria
□ Research type: Not limited by research type or research design. □ Research object: Participants included children and adolescents between the ages of 1 and 18 years, cases with positive nucleic acid tests in patients with COVID-19. □Intervention was unrestricted. □ Outcomes included clinical manifestations, laboratory examinations, and CT examinations.
1.2.2 Exclusion criteria
□ Infants less than 1 year of age. □ Fewer than 4 cases reported. □ Surveillance reports, community outbreaks, review papers, commentary articles, conference papers, duplicated reports, reports for which the full text cannot be obtained. □ There is no definite measure or laboratory marker for the diagnosis of COVID-19. □ The outcome was not clear.
1.3 Data extraction
Two researchers (HZ, LL) independently screened and cross-checked the literature regarding the inclusion and exclusion criteria. Any disagreement was resolved by discussion between the two reviewers. A customized form was used to record the first author, publication time, design of the trial, country, the number of COVID-19 patients, ages, sexes, durations between onset of symptoms and hospitalization (days), times of patient examinations, diagnostic criteria for COVID-19, clinical symptoms, laboratory outcomes, chest CT findings, and supportive treatment. In addition, we screened them according to whether blood or respiratory samples were positive by real-time polymerase chain reaction tests for SARS-CoV-2 nucleic acid.
1.4 Quality assessment of included meta-analyses
For the case series study, we used the Quality Assessment Tool for Case Series Studies to evaluate article suitability for systematic review [9]. Each item was scored as either 0 or 1 point based on the scoring criteria, and scores were summed across items to generate an overall quality score ranging from 0 to 9. Overall scores were classified as low risk (≥7 points), moderate risk (5–6 points), or high risk (0–4 points). Two evaluators (HZ, LL) separately performed quality assessment. Any disagreements were resolved through discussion among the investigators.
1.5 Statistical analysis
Meta-analysis was performed using STATA 14.0. A random-effects model was used to compute the combined prevalence and 95% confidence intervals (CI). We calculated the pooled incidence of clinical symptoms, laboratory findings, and chest CT findings. Heterogeneity was assessed using Cochran’s Q test with a significance level of p < 0.1 and quantified using the I2 statistic. Heterogeneity was quantified using the I-squared (I2) statistic and categorized as low (I2 <25%), moderate (I2=25-50%) or high (I2 >50%). A model of fixed effect (FE) was set with 95% CI if no statistical evidence of heterogeneity existed (p≥ 0.1, I2 ≤ 50%), while a model of random effect (RE) was applied to estimate pooled effect with 95% confidence intervals (CI) if statistical heterogeneity was found (p < 0.1, I2 > 50%). If significant heterogeneity (p< 0.1, I2 > 75%) was detected, we used sensitivity analysis to explore its possible sources. A random-effects model was used if the reason for heterogeneity could not be identified. Publication bias was detected using Begg’s test. Probability (p) values less than 0.05 were considered statistically significant.
2 Results
2.1 Systematic search results
The search strategy initially identified 467 publications, including 60 from PubMed, 131 from Embase, 5 from Cochrane, and 196 from Web of Science. Search results from different sources were entered into an EndNote library, from which 146 duplicates and 366 irrelevant studies were removed. Among the remaining 101 articles selected for full-text reading, 52 studies were removed. Finally, 49 studies [10–58] were included in the meta-analysis involving 1627 participants. Only three of 49 included studies reported critically ill patients [15,26,31]. These critically ill patients were not excluded from the meta-analysis. Mechanical ventilation analysis included only critically ill patients. We extracted data based on different outcome indicators and then conducted a single-arm meta-analysis. Figure 1 illustrates the detailed process of the literature review.

Flow chart of literature search and selection of studies.
2.2 Study characteristics
The characteristics of the studies are displayed in Table 1. The studies included were published between February 26, 2020 and June 29, 2020. Fifty articles including 41 (84%) English papers and 8 (16%) Chinese papers were included in our study, and all were journal articles. Patients were from six countries: 41 from China, 4 from the United States, 1 from Italy, 1 from France, 1 from Turkey, and 1 from Iran. All included studies were retrospective studies; one was a case-control study, and the remainder were retrospective case series. The number of patients enrolled in each study ranged from 4 to 157, and patients’ ages ranged from 1 to 18 years. Male patients accounted for 53%, and female patients accounted for 47%. All patients were confirmed to be positive for SARS-CoV-2 nucleic acid by respiratory or blood sample.
2.3 Methodological assessment of the included literature
For the evidence of effectiveness meta-analysis, we used the Quality Assessment Tool for Case Series Studies to evaluate article suitability for the systematic review. Among the 49 studies included, 43 studies were rated as low risk of bias, 6 studies as moderate, and none were rated as high risk of bias (Table 2).
2.4 Meta-analysis results
We meta-analyzed the prevalence of 18 clinically relevant symptoms (Table 3), the prevalence of 12 laboratory outcomes (Table 4), and the prevalence of 9 chest CT findings (Table 5). The analysis of the 48 articles included showed that boys (53% [0.50−0.56]) had a higher prevalence of COVID-19 than did girls (47% [0.44−0.50]).
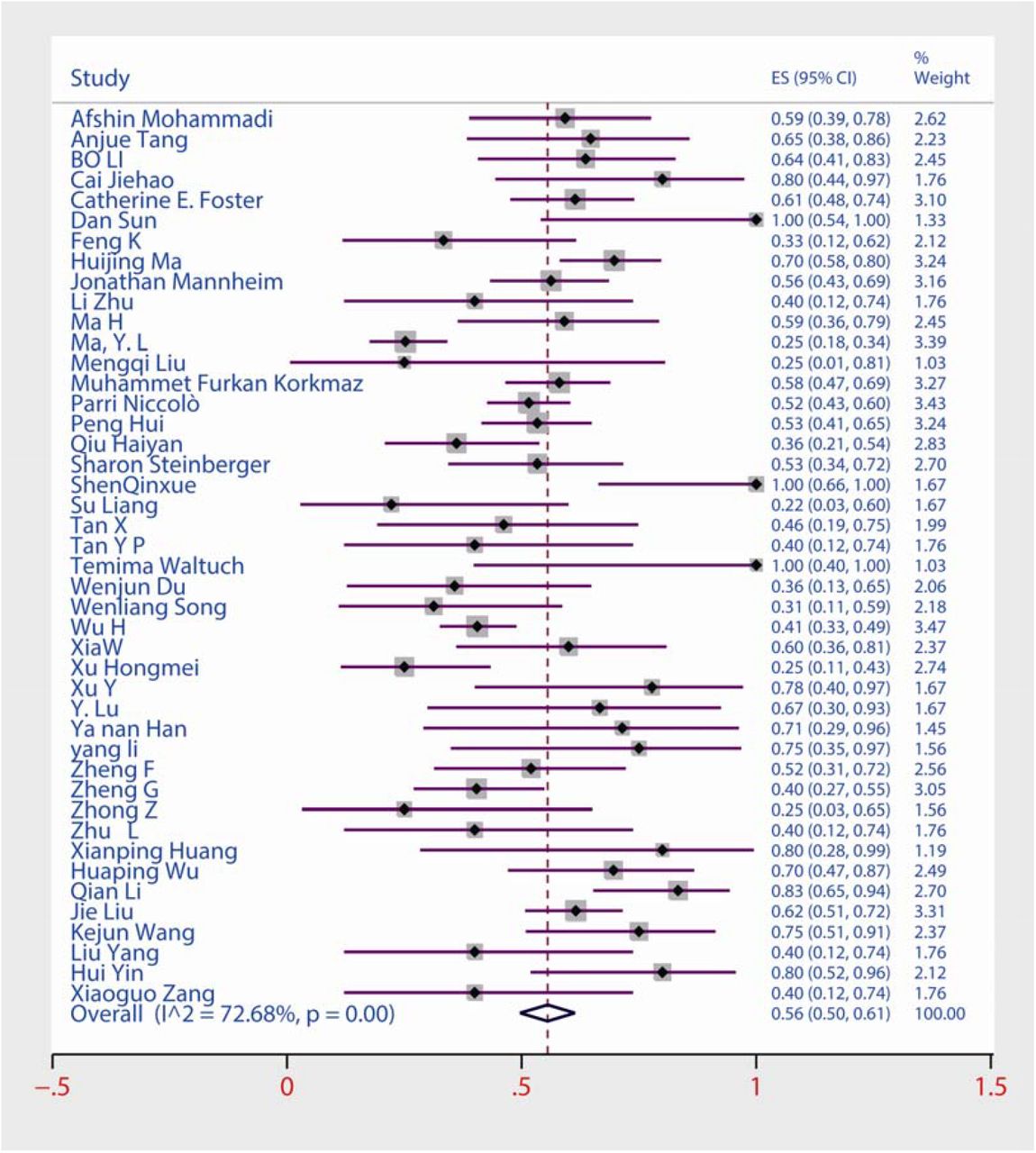
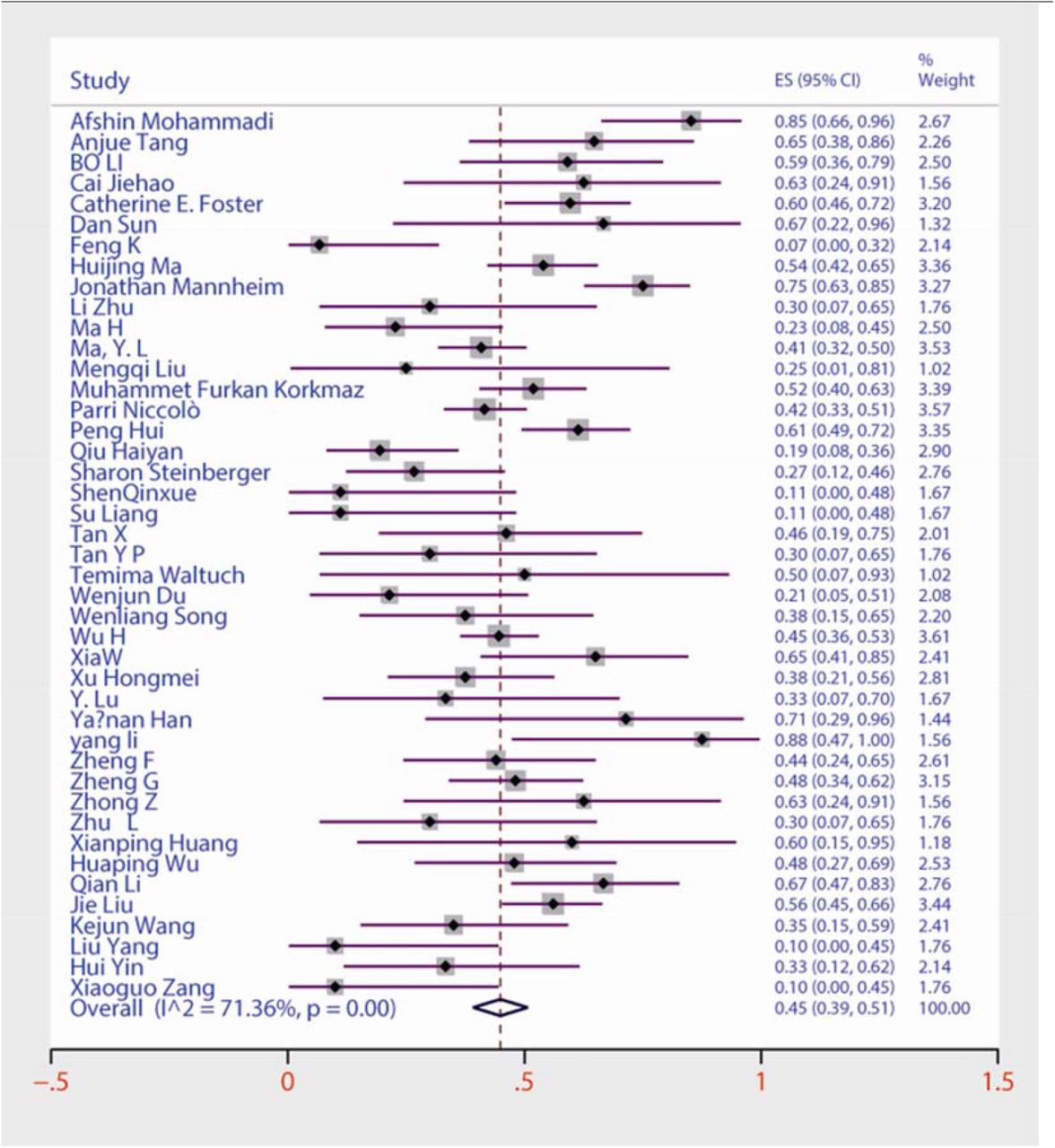
Among the 18 frequently reported clinical symptoms (Table 3), the incidence of clinical symptoms of COVID-19 in children and adolescents was 86% [95% CI 0.77−0.93], and the most common clinical symptoms were fever (56% [0.50−0.61]) (Supplementary Figs S 1), cough (45% [0.39−0.51]) (Supplementary Figs S 2), sneezing (14% [0.08−0.22]), and vomiting (14% [0.06−0.24]). Other symptoms included diarrhea (12% [0.06−0.19]), anhelation (11% [0.04−0.19]), sore throat (10% [0.05−0.16]), headache (10% [0.04−0.17]), fatigue (9% [0.05 −0.15]), myalgia (8% [0.02−0.17]), increased sputum volume (7% [0.03−0.13]), and abdominal pain (6% [0.01−0.12]). In addition, the meta-analysis included 3 studies with critically ill children and showed that the incidence of mechanical ventilation in severely ill children was 38% [0.27−0.50]. All the above results were statistically significant (p□<□0.05). There was no statistical significance (P>0.05) for the analyzed results for renal insufficiency or mortality. Of the 49 included studies, only 3 case studies of critically ill children reported deaths, and no deaths were reported in the remaining 47 studies. Publication bias was found for symptoms of sore throat, anhelation, headache, diarrhea, and vomiting, and no publication bias was found for the remaining clinical symptoms.
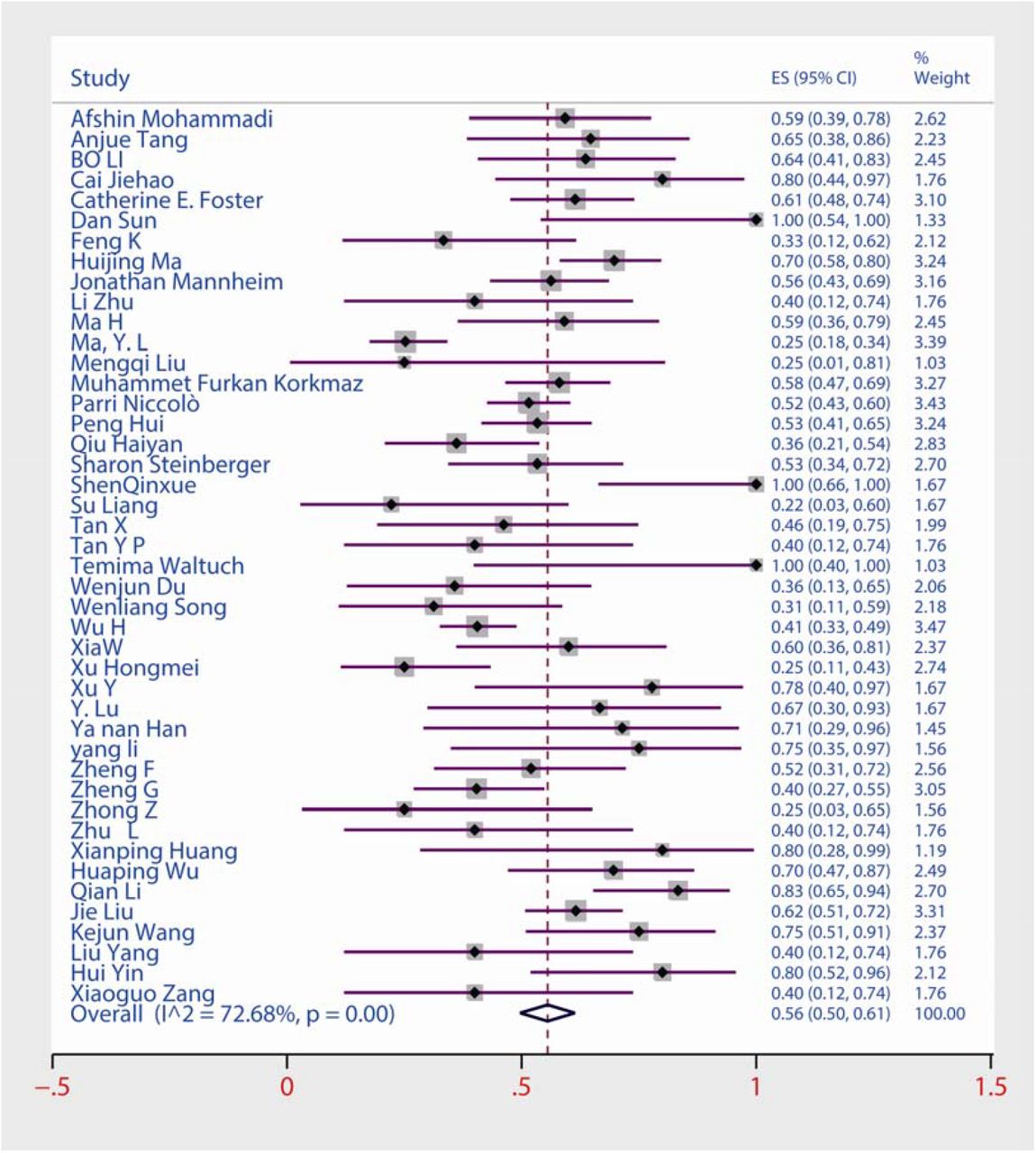
Forest plots of the prevalence of fever among children and adolescents with COVID-19.

Forest plots of the prevalence of cough among children and adolescents with COVID-19.
Among the 13 frequently reported laboratory findings (Table 4), the most common abnormalities in laboratory examinations were elevated procalcitonin (40% [0.23−0.57]), elevated lactate dehydrogenase (31% [0.19−0.43]), increased lymphocyte count (28% [0.17−0.42]), increased creatine kinase (28%[0.18−0.40]), and elevated C-reactive protein (26% [0.17−0.36]) (Supplementary Figs S 3, 4, 5, 6 and 7). Additional laboratory findings included elevated AST (24%[ 0.09−0.43]), decreased leukocyte count (21% [0.13−0.29]), elevated D-dimer (19% [0.09−0.31]), reduced lymphocyte count (15% [0.09−0.21]), increased leukocyte count (15% [0.07−0.25]), and elevated ALT (7% [0.05−0.10]). Because only two studies reported elevated creatinine, we did not perform a meta-analysis. All the results described above were statistically significant (p□<□0.05). Begg’s test indicated significant publication bias for decreased leukocyte count, elevated ALT, and elevated D-dimers, and no remaining laboratory findings showed significant publication bias at p < 0.05.
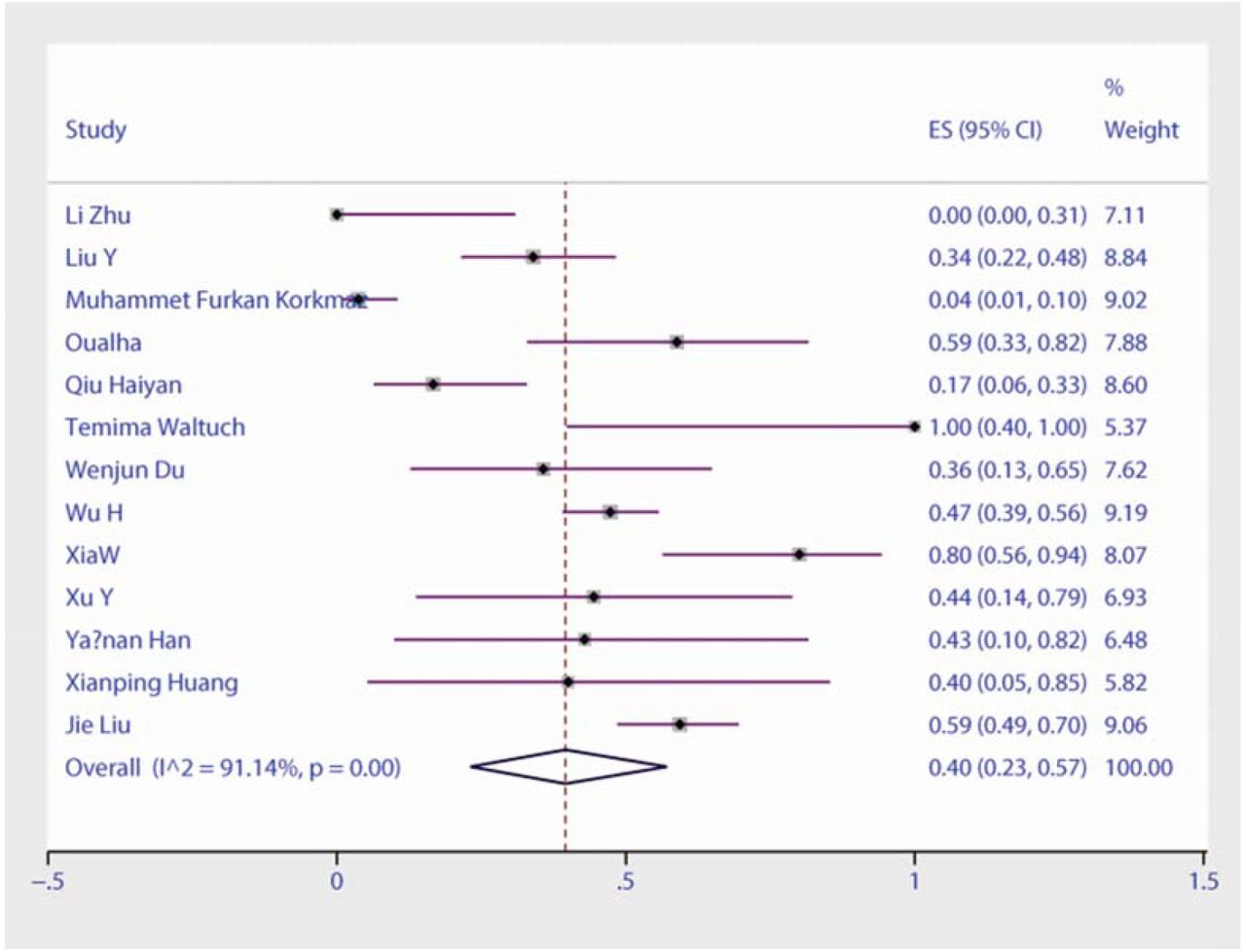
Forest plots of the prevalence of elevated procalcitonin among children and adolescents with COVID-19.

Forest plots of the prevalence of elevated lactate dehydrogenase among children and adolescents with COVID-19.
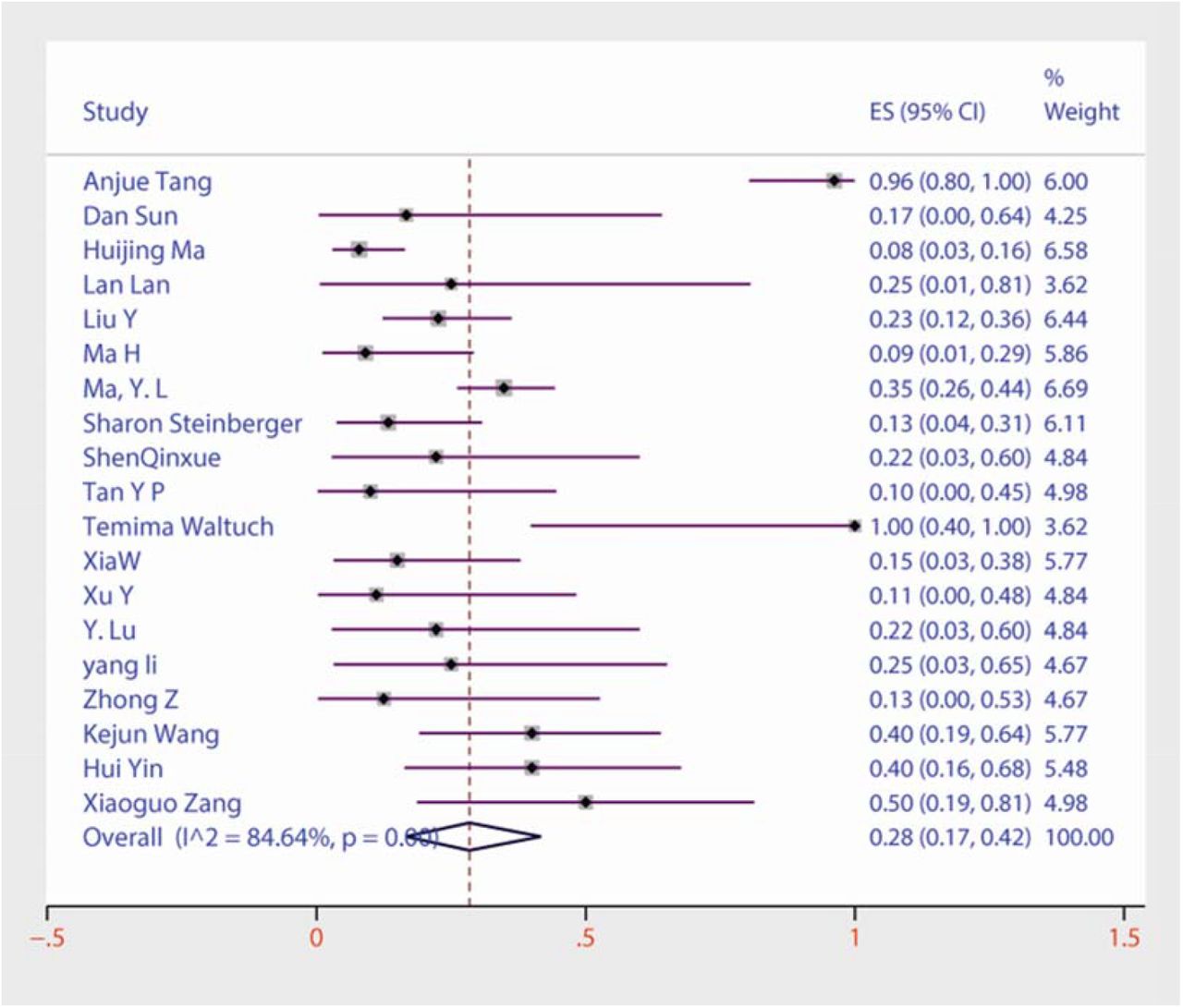
Forest plots of the prevalence of increased lymphocyte count among children and adolescents with COVID-19.

Forest plots of the prevalence of increased creatine kinase among children and adolescents with COVID-19.

Forest plots of the prevalence of C-reactive protein among children and adolescents with COVID-19.
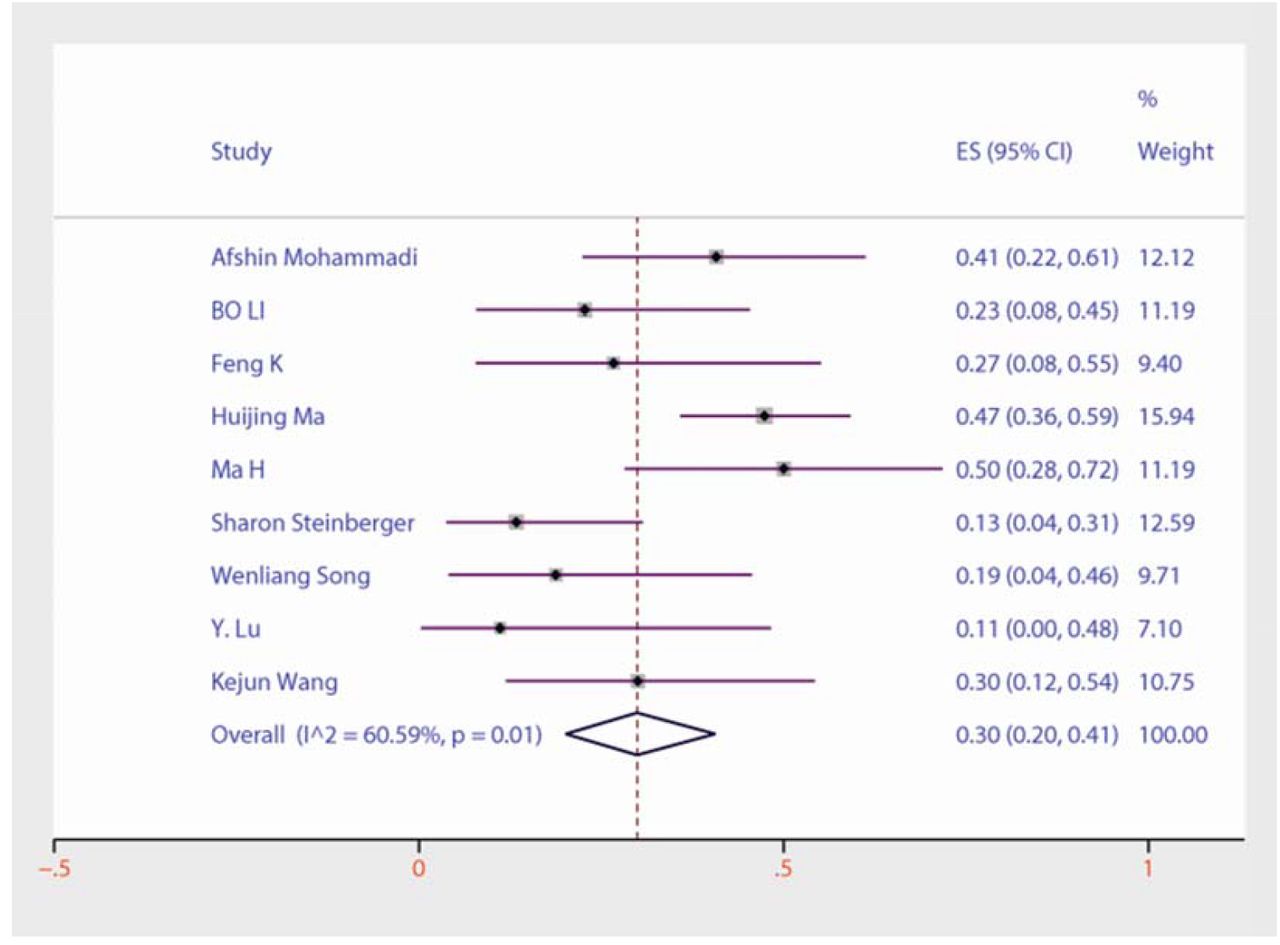
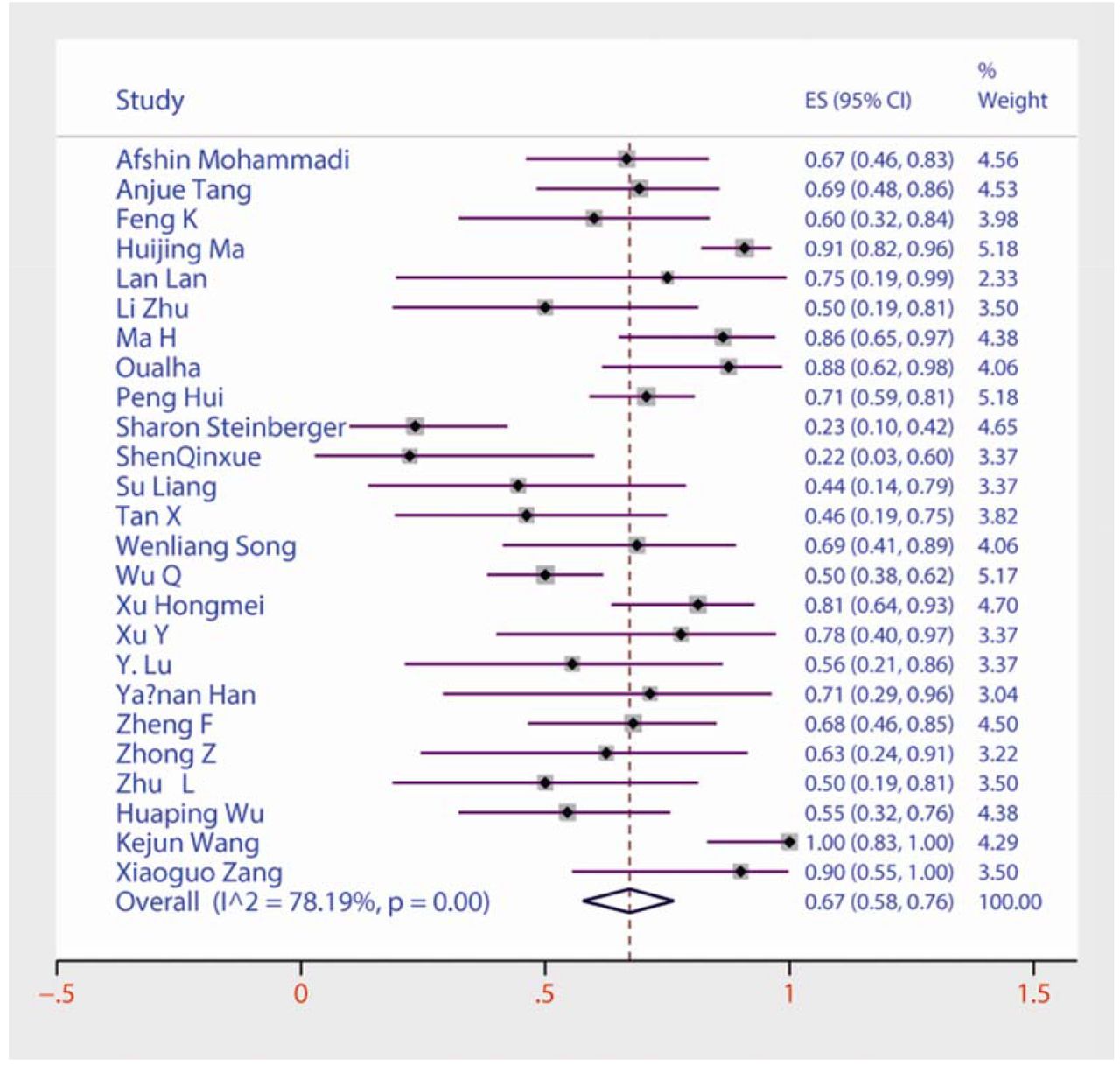
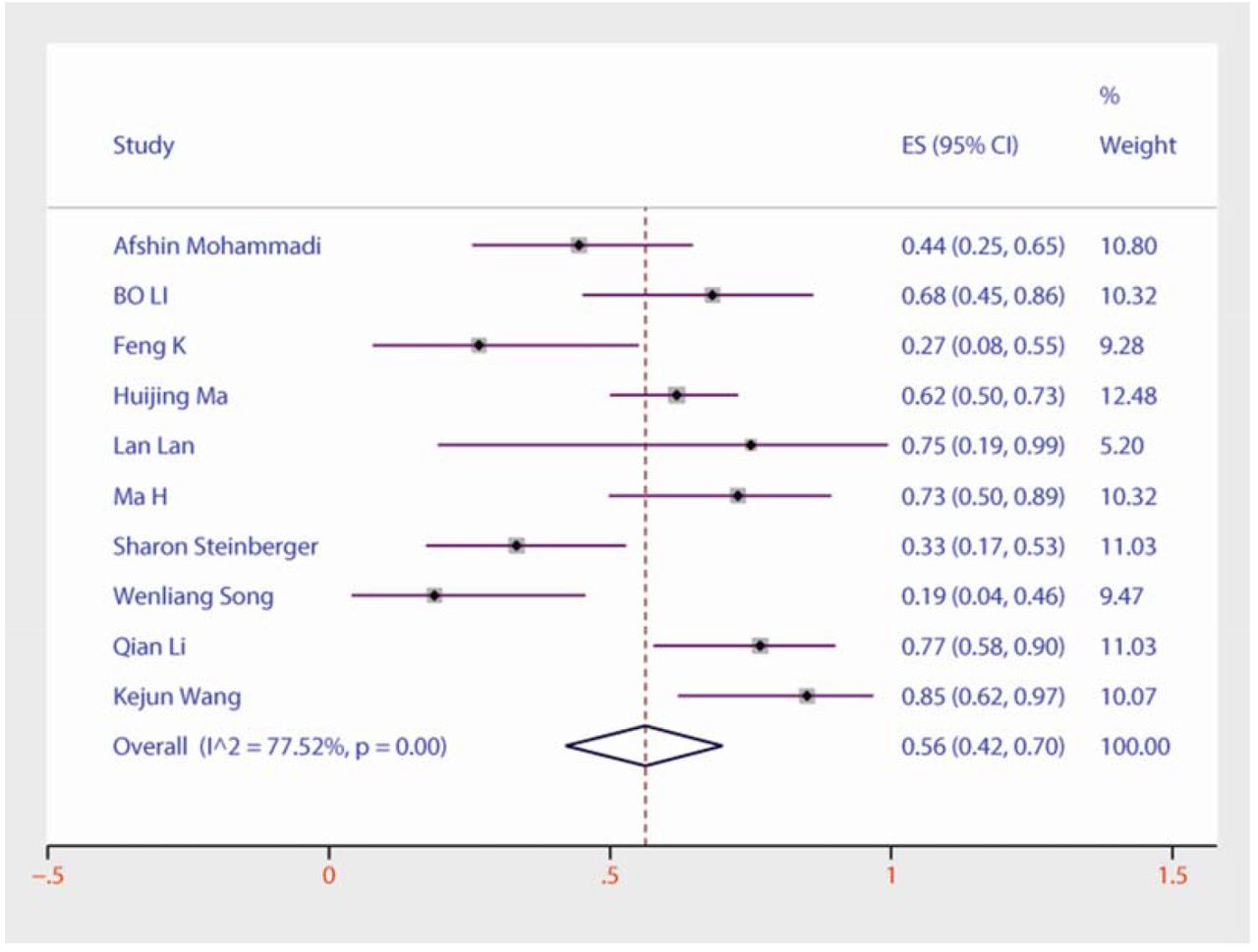
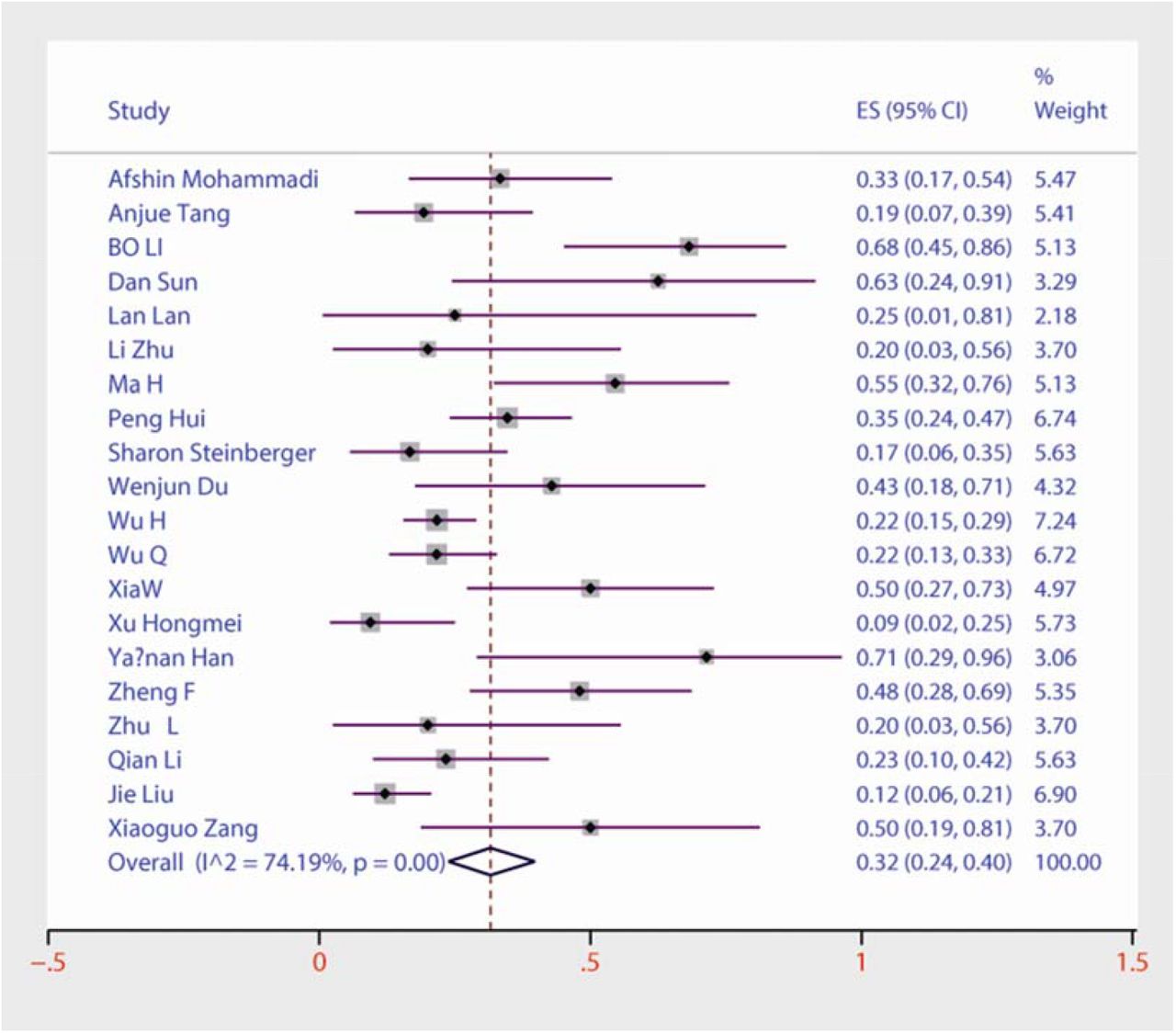
Among the 9 frequently reported chest CT findings (Table 5), in the included 26 studies, the prevalence of chest CT examinations showing infection was 67% [0.58−0.76] (Supplementary Figs S 8). The most common abnormalities from chest CT examination were lower lobe involvement (56% [0.42-0.70]), ground-glass opacities (33% [0.25−0.42]), bilateral pneumonia (32% [0.24-0.40]), patchy shadows (31% [0.18-0.45]), and upper lobe involvement (30% [0.20-0.41]) (Supplementary Figs S 9, 10, 11, 12 and 13). Other outcomes included unilateral pneumonia (26% [0.22-0.30]), tubercles (13% [0.06-0.21]), pleural fluid (3% [0.00-0.08]). All the abovementioned results were statistically significant (p□<□0.05). Publication bias was found for bilateral pneumonia, and there was no evidence of significant publication bias among the remaining 9 included studies.
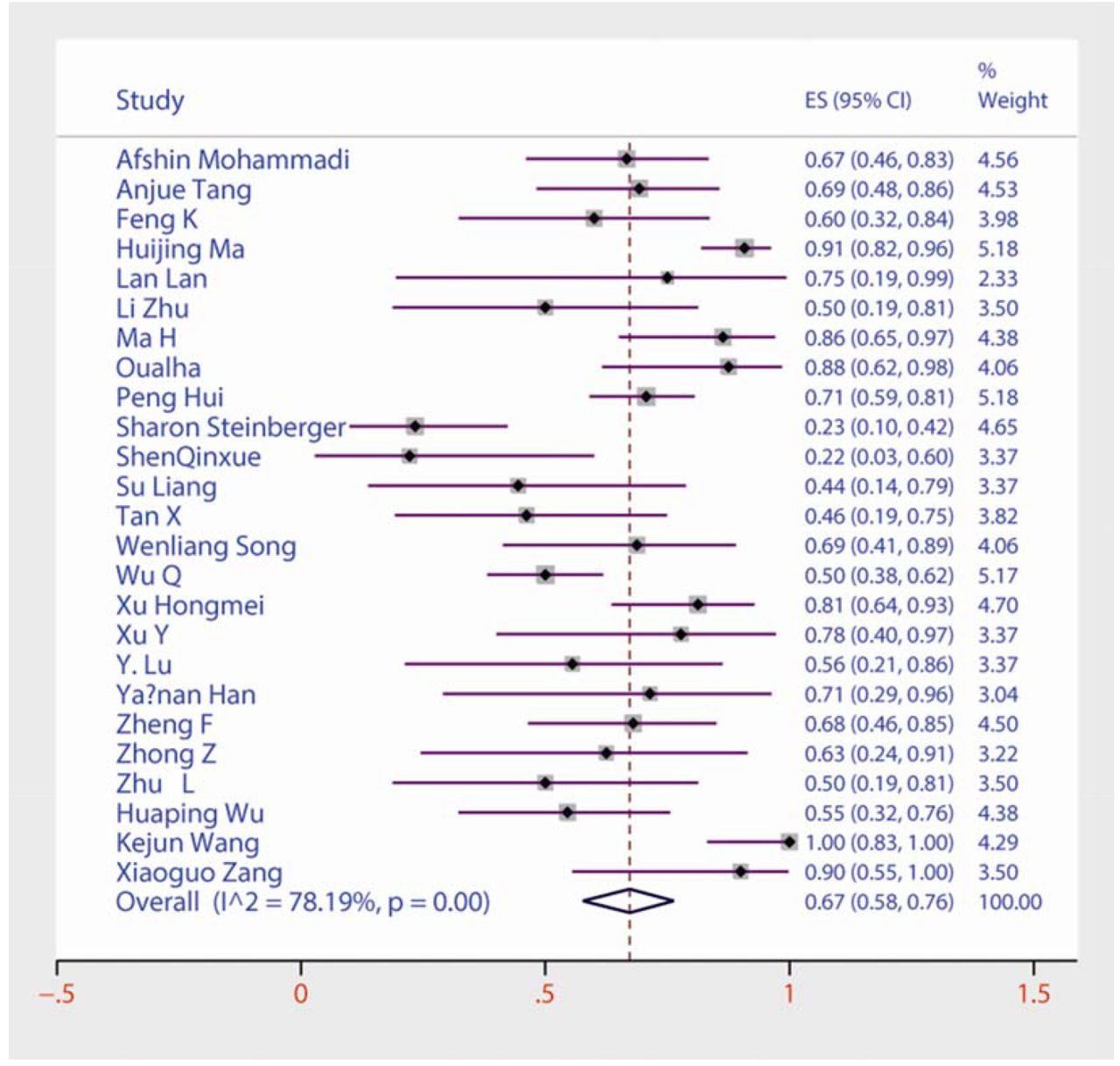
Forest plots of the prevalence of chest CT examinations showing infection among children and adolescents with COVID-19.
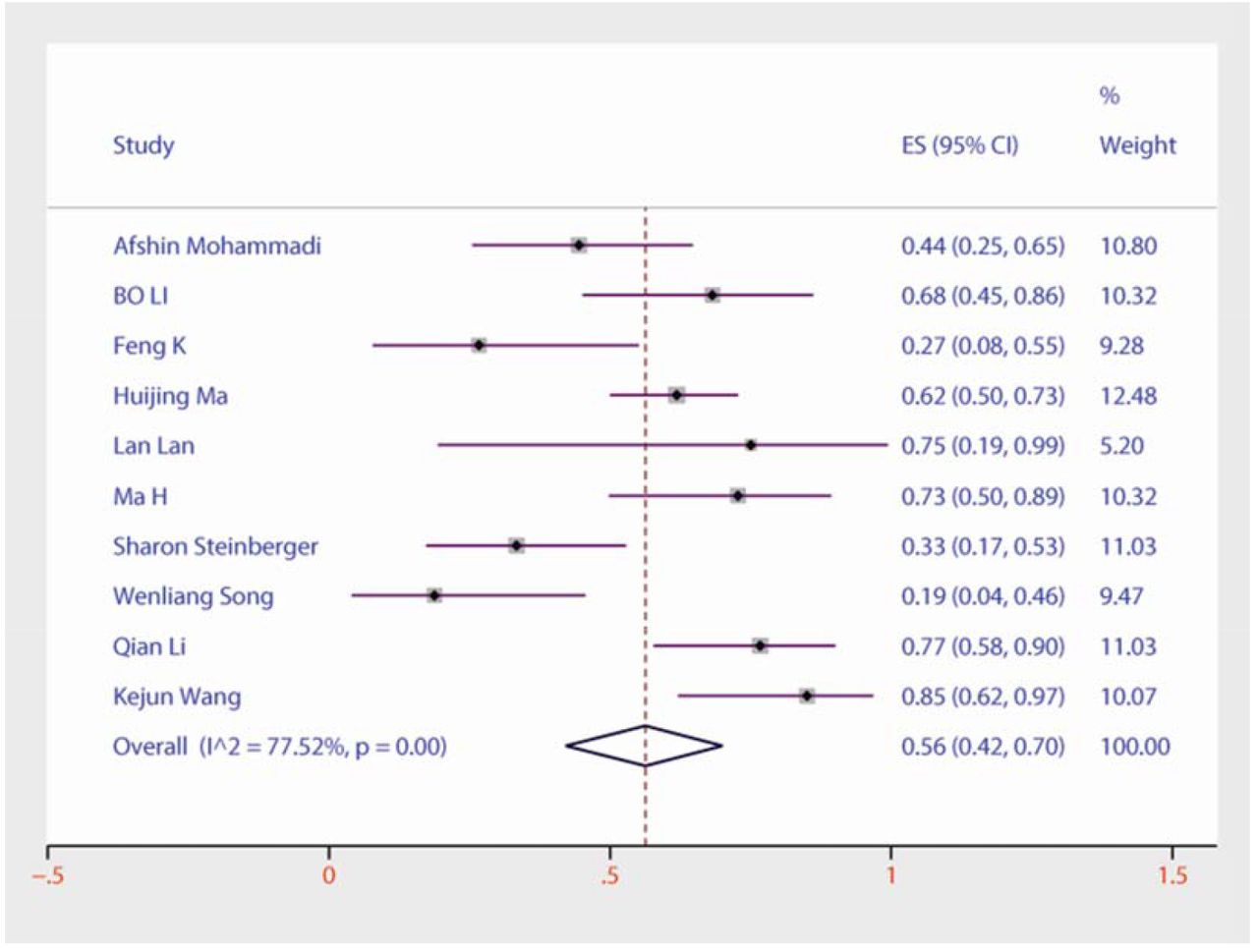
Forest plots of the prevalence of lower lobe involvement among children and adolescents with COVID-19.

Forest plots of the prevalence of ground-glass opacities among children and adolescents with COVID-19.

Forest plots of the prevalence of bilateral pneumonia among children and adolescents with COVID-19.

Forest plots of the prevalence of patchy shadows among children and adolescents with COVID-19.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Forest plots of the prevalence of upper lobe involvement among children and adolescents with COVID-19.
3 Discussion
This meta-analysis summarizes the latest and most comprehensive study for clinical characteristics of COVID-19 in children and adolescents, from the first report of COVID-19 to July 10, 2020, including clinical features, laboratory outcomes, and chest CT findings. We conducted a systematic review and meta-analysis of 49 studies involving 1627 patients. The proportion of boys was significantly higher than that of girls, also consistent with previous studies, according to the synthesis results of our meta-analysis. Compared with the two previous systematic reviews on this topic, we have included more studies and analyzed 40 results in detail.
The main clinical features in children and adolescents with COVID-19 were fever (56%), cough (45%), sneezing (14%), vomiting (14%), and other less common results included diarrhea (12%), anhelation (11%), sore throat (10%), headache (10%), fatigue (9%), myalgia (8%), increased sputum volume (7%), and abdominal pain (6%). According to a previous study of COVID-19 in adult patients, the main clinical features of COVID-19 were fever, cough, and fatigue [59–60]. In this study of children and adolescents, patients with symptoms of sneezing and vomiting also accounted for reasonably large percentages. Previous studies have found that nasal congestion, runny nose and diarrhea were less common in children than in adults [61–63]. Critical or fatal pediatric COVID-19 cases were rare, and children with COVID-19 showed less severe clinical symptoms than did adults. In addition, one study showed that children may be less likely to be infected, and may show milder symptoms if they are infected [63]. Therefore, children and adolescents are more likely to have potential hidden infections, which should attract the attention of clinicians and parents of children.
The most common laboratory abnormalities were elevated procalcitonin (40%), elevated lactate dehydrogenase (31%), increased lymphocyte count (28%), elevated creatine kinase (28%) and elevated C-reactive protein (26%). These laboratory abnormalities indicate clear viral infection. Previous studies have found the most common laboratory test abnormalities in adult patients to be elevated C-reactive protein and reduced lymphocyte count [59–60]. All these abnormal laboratory markers are nonspecific, so their clinical applications are limited. According to the findings of our study, the elevated procalcitonin, elevated lactate dehydrogenase and increased lymphocyte count may appear as nonspecific markers in children and adolescents. Previous research has suggested that mortality, acute respiratory distress syndrome (ARDS), headache, increased leukocyte count, and elevated lactate dehydrogenase are significantly higher in studies with a larger proportion of older patients [59]. When evaluating suspicious cases, doctors cannot rely on these laboratory abnormalities to rule out or confirm the diagnosis of COVID-19 [59]. One study suggested that these abnormalities may be related to the cytokine storm caused by infection [64]. Recently, another study revealed that COVID-19 might mainly affect T lymphocytes, especially CD4+T cells, resulting in significant lymphopenia [65].The results of this study showed that the prevalence of increased lymphocyte count in children (28%) was higher than the prevalence of decreased lymphocyte count (15%), which may be related to the percentage of lymphocytes elevated in the growth and development of the child’s immune system. In terms of liver enzymes, elevated AST (24%) was more common than elevated ALT (7%), which indicates that liver function may be damaged to varying degrees. In addition, reduced leukocyte count (21%) was more common than increased leukocyte count (15%). Of the 49 studies reviewed, only two reported elevated creatinine. Therefore, elevated creatinine was extremely rare among children with COVID-19.
Chest CT examination was one of the important auxiliary examinations for COVID-19 pneumonia, and it has a very satisfactory effectiveness for the examination of lung lesions. Previous research has found that most patients have mild symptoms and elevated body temperature, but pulmonary lesions are relatively obvious. Li [66] found that chest CT had a low rate of missed diagnosis of COVID-19 (3.9%) and could thus be used as a rapid diagnostic method for this disease to optimize patient management. However, CT is still limited in identifying specific viruses and distinguishing viruses. Our meta-analysis showed that the prevalence of children and adolescents with COVID-19 chest CT examinations showing infection was 67%. A recent study of 62 adult patients with COVID-19 showed that 52 (83.9%) had an abnormal chest CT scan, which was much higher than the frequency in children and adolescents with an abnormal chest CT scan, consistent with previous reports [67]. The results of our meta-analysis showed that the prevalence of ground-glass opacity and patchy shadows were 33% and 31%, respectively. Lung lesions of patients with COVID-19 showed imageology findings similar to those of other viral pneumonia, mainly ground-glass opacities and patchy shadows. The most common position for lesions detected by CT scan was in the lower lobe (56%), while incidence of upper lobe lesion was 30%. Bilateral pneumonia (32%) was more common than unilateral pneumonia (26%). A study of adult COVID-19 patients showed that bilateral pneumonia was present in 73.2% of cases, indicating that adults are more likely to experience bilateral lung infection than are children and adolescents [59]. The results of this study found that tubercles (13%) and pleural fluid (3%) rarely occur in children and adolescents with COVID-19. Chang et al. found that, compared with SARS, COVID-19 has prominent characteristics in children, and the typical appearance of chest CT is ground-glass opacity, which is also consistent with our study [68]. Other CT findings, such as air bronchogram and lymphadenopathy, are less common [69].
Among the 49 articles included, only 3 studies of critically ill children reported deaths. Among the 1627 patients included, only 7 deaths occurred, and the overall mortality was lower than the reported adult mortality (3.6%) [59]. Compared with other common viral diseases, the number of cases of COVID-19 in children and adolescents is small, and the mortality is low, which is very gratifying.
There are also several limitations to our systematic review and meta-analysis. First, all reported cases were retrospective studies, and there was a high degree of heterogeneity among the results of the study. Because there were many studies included, it is difficult to avoid heterogeneity. No subgroup analysis was performed on different age groups of the included children and adolescents. Second, the current COVID-19 pandemic has not been effectively controlled. Our study was analyzed during the COVID-19 outbreak. Most of the included patients were from China, and there may be certain geographical and ethnic differences. Subgroup analysis was not performed, which may also bias the results of the analysis.
4 Conclusion
This meta-analysis provides a comprehensive review of the clinical characteristics of COVID-19 in children and adolescents. The main clinical features of children and adolescents were fever and cough. The most frequently reported laboratory abnormalities were elevated procalcitonin, elevated lactate dehydrogenase, increased lymphocyte count, increased creatine kinase, and elevated C-reactive protein. From chest computed tomography, the most common lesion site was the lower lobe. Bilateral pneumonia was more common than unilateral pneumonia, and the main manifestations were ground-glass opacities and patchy shadowing. The condition of children and adolescents with COVID-19 was milder than that of adult patients, with a greater proportion of asymptomatic and mild cases, and specific diagnosis and source-of-infection control were more challenging.
Data Availability
All data generated or analyzed during this study are included in this article.
Declarations
Ethics approval and consent to participate
Not applicable. This article does not contain any studies with human participants performed by any of the authors.
Consent for publication
All participating authors provide consent for publication.
Availability of data and materials
All data generated or analyzed during this study are included in this article.
Competing interests
The authors declare that they have no competing interests.
Funding
The authors state that this work has not received financial support.
Authors’ contributions
All the authors designed the study. LL, HZ, ZL and BT designed the literature search and searched the articles. LL, HZ, ML, YC, JL, and BT contributed to statistical analysis, interpretation of data and data review. LL and HZ wrote the first draft of the article. All the authors revised the article and approved the final version.
Acknowledgements
Not applicable.
Footnotes
Email:loulixiang{at}qq.com, Email:zhanghui10157{at}163.com, Email:18697126038{at}163.com, Email:865880047{at}qq.com, Email:lzq611206771{at}163.com, Email:1736853849{at}qq.com, Email:543715871{at}qq.com, Email:chongyuliang{at}163.com
Competing interests: No authors have competing interests in this research.
Funding: This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Contributors: All the authors designed the study. LL, HZ, ZL and BT designed the literature search and searched the articles. LL, HZ, ML, YC, JL, and BT contributed to statistical analysis, interpretation of data and data review. LL, HZ wrote the first draft of the article. All the authors revised the article and approved the final version.
References
- [1].↵
- [2].↵
- [3].↵
- [4].↵
- [5].↵
- [6].↵
- [7].↵
- [8].↵
- [9].↵
- [10].↵
- [11].
- [12].
- [13].↵
- [14].
- [15].↵
- [16].
- [17].
- [18].
- [19].
- [20].
- [21].
- [22].
- [23].
- [24].
- [25].
- [26].↵
- [27].
- [28].
- [29].
- [30].
- [31].↵
- [32].
- [33].
- [34].
- [35].
- [36].
- [37].
- [38].
- [39].
- [40].
- [41].
- [42].
- [43].
- [44].
- [45].
- [46].
- [47].
- [48].
- [49].
- [50].
- [51].
- [52].
- [53].
- [54].
- [55].
- [56].
- [57].
- [58].↵
- [59].↵
- [60].↵
- [61].↵
- [62].
- [63].↵
- [64].↵
- [65].↵
- [66].↵
- [67].↵
- [68].↵
- [69].↵




