
ABSTRACT
Background Several studies have reported a reduced risk of death associated with the inpatient use of angiotensin receptor blockers (ARBs) and angiotensin converting enzyme inhibitors (ACEIs) in COVID-19 patients, but have been criticized for incurring in several types of bias. Also, most studies have pooled ACEIs and ARBs as if they were a unique group, overlooking their pharmacological differences. We aimed to assess whether the in-hospital continuation of ARBs and ACEIs, in regular users of these drugs, was associated with a reduced risk of death as compared to their discontinuation and also to compare head-to-head ARBs with ACEIs.
Methods Adult patients with a PCR-confirmed diagnosis of COVID-19 requiring admission during March, 2020 were consecutively selected from 7 hospitals in Madrid, Spain. Among them, we identified outpatient users of ACEIs/ARBs and divided them in two cohorts depending on treatment discontinuation/continuation at admission. Then, they were followed-up until discharge or in-hospital death. An intention-to-treat survival analysis was carried out and hazard ratios (HRs) and their 95%CI were computed through a Cox regression model adjusted for propensity scores of discontinuation and controlled by potential mediators.
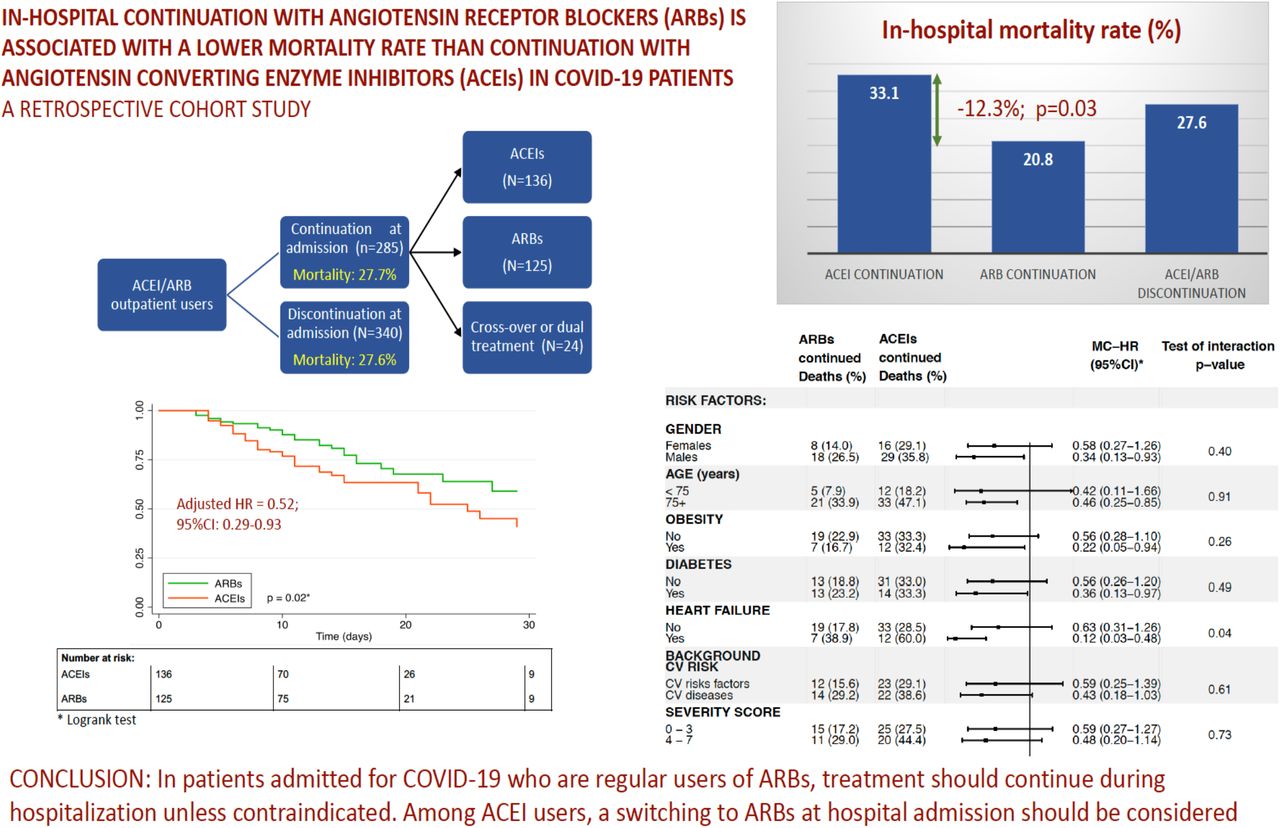
Results Out of 625 ACEI/ARB users, 340(54.4%) discontinued treatment. The in-hospital mortality rates were 27.6% and 27.7% in discontinuation and continuation cohorts, respectively (HR=1.01; 95%CI:0.70-1.46). No difference in mortality was observed between ARB and ACEI discontinuation (28.6% vs. 27.1%, respectively), while a significantly lower mortality rate was found among patients who continued with ARBs (20.8%,N=125) as compared to those who continued with ACEIs (33.1%,N=136; p=0.03). The head-to-head comparison (ARB vs. ACEI continuation) yielded an adjusted HR of 0.52 (95%CI:0.29-0.93), being especially notorious among males (HR=0.34; 95%CI:0.12-0.93), subjects older than 74 years (HR=0.46; 95%CI:0.25-0.85), and patients with obesity (HR=0.22; 95%CI:0.05-0.94), diabetes (HR=0.36; 95%CI:0.13-0.97) and heart failure (HR=0.12; 95%CI:0.03-0.97).
Conclusions Among regular users of ARBs admitted for COVID-19, the in-hospital continuation with them was associated with an improved survival, while this was not observed with ACEIs. Regular users of ARBs should continue with this treatment if admitted for COVID-19, unless medically contraindicated. In admitted ACEI users, a switching to ARBs should be considered, especially among high-risk patients.

{kind=link}
Competing Interest Statement
The authors have declared no competing interest.
Funding Statement
Funding: This study is part of a larger project which received funding from the Instituto de Salud Carlos III (#COV20/00027). Additionally, the University of Alcala (#COVID-19 UAH 2019/00003/016/001/028) and the Biomedical Research Foundation from the University Hospital Principe de Asturias granted to FdA complementary grants for this project. The funding sources had no role in the study design, data collection, analysis and interpretation of data, writing of the report; and in the decision to submit the paper for publication.
Author Declarations
I confirm all relevant ethical guidelines have been followed, and any necessary IRB and/or ethics committee approvals have been obtained.
Yes
The details of the IRB/oversight body that provided approval or exemption for the research described are given below:
The present study was an extension of a previous study approved by the Ethics Research Committee of the University Hospital Principe de Asturias on March 18, 2020 (#SRAA-COVID19), including a waiver for the informed consent [6]. The Ethics Research Committee was informed of this extension, and no additional ethical assessment was required. Data extracted were fully anonymised and no attempt was made to interview patients or relatives. The study complied with the provisions of the European and Spanish legislation.
All necessary patient/participant consent has been obtained and the appropriate institutional forms have been archived.
Yes
I understand that all clinical trials and any other prospective interventional studies must be registered with an ICMJE-approved registry, such as ClinicalTrials.gov. I confirm that any such study reported in the manuscript has been registered and the trial registration ID is provided (note: if posting a prospective study registered retrospectively, please provide a statement in the trial ID field explaining why the study was not registered in advance).
Yes
I have followed all appropriate research reporting guidelines and uploaded the relevant EQUATOR Network research reporting checklist(s) and other pertinent material as supplementary files, if applicable.
Yes
Footnotes
↵* MED-ACE2-COVID19 Study Group: Hospital Universitario Príncipe de Asturias: F J de Abajo, A Rodríguez-Miguel, S Rodríguez-Martín, V Lerma, A García-Lledó, D Barreira-Hernández; D Rodríguez-Puyol; Hospital Universitario de Getafe: O Laosa, L Pedraza, L Rodríguez-Mañas; Hospital Universitario Ramón y Cajal: M Aguilar, I de Pablo, MA Gálvez; Hospital Central de la Defensa Gómez Ulla: A García-Luque, M Puerro; RM Aparicio, V García-Rosado, C Gutiérrez-Ortega; Hospital Clínico San Carlos: L Laredo, E González-Rojano, C Pérez, A Ascaso, C Elvira; Hospital Universitario de La Princesa: G Mejía-Abril, P Zubiaur, E Santos-Molina, E Pintos-Sánchez, M Navares-Gómez; F Abad-Santos; Hospital Universitario Puerta de Hierro-Majadahonda: G A Centeno, A Sancho-Lopez, C Payares-Herrera, E Diago-Sempere.
Data Availability
Data sharing: After publication, the data will be made available to others on reasonable requests to the corresponding author. A proposal with detailed description of study objectives and statistical analysis plan will be needed for evaluation of the reasonability of requests. Additional materials might also be required during the process of evaluation. Deidentified participant data will be provided after approval from the principal researchers of the participating hospitals.
ABBEVIATIONS
- ACE1
- Angiotensin converting enzyme 1
- ACE2
- Angiotensin converting enzyme 2
- ACEIs
- Angiotensin-converting enzyme inhibitors
- AMRs
- Antagonists of mineralocorticoid receptor
- ARBs
- Angiotensin receptor blockers
- AT1R
- Receptor for angiotensin II type 1
- AT2R
- Receptor for angiotensin II type 2
- BMI
- Body mass index
- CCBs
- Calcium channel blockers
- CI
- Confidence interval
- COPD
- Chronic obstructive pulmonary disease
- COVID-19
- Coronavirus disease 19
- CPR
- C-protein reactive
- CV
- Cardiovascular
- ED
- Emergency Department
- HR
- Hazard ratio
- ICU
- Intensive care unit
- IQR
- Interquartile range
- ITT
- Intention-to-treat
- MC-HR
- Mediator-controlled hazard ratio
- NSAIDs
- Nonsteroidal anti-inflammatory drugs
- NT-pro-BNP
- N terminal pro-peptide of natriuretic factor type B
- OADs
- Other antihypertensive drugs different from RASIs or CCBs
- OR
- Odds ratio
- PS
- Propensity scores
- PS-adjusted HR
- Propensity score adjusted hazard ratio
- RASIs
- Renin-angiotensin system inhibitors
- SD
- Standard deviation




