
Abstract
Background It is unclear whether smoking increases the risk of COVID-19 hospitalisation. We aimed to i) examine the association of smoking status with hospitalisation for COVID-19 compared with hospitalisation for other respiratory virus infections a year previous; ii) compare current smoking in cases with age- and sex-matched London prevalence; and iii) examine concordance between smoking status recorded on the electronic health record (EHR) and the medical notes.
Methods This retrospective case-control study enrolled adult patients (446 cases and 211 controls) at a single National Health Service trust in London, UK. London smoking prevalence was obtained from the representative Annual Population Survey. The outcome variable was type of hospitalisation (COVID-19 vs. another respiratory virus). The exposure variable was smoking status (never/former/current smoker). Logistic regression analyses adjusted for age, sex, socioeconomic position and comorbidities were performed. The study protocol and analyses were pre-registered on the Open Science Framework.
Findings Patients hospitalised with COVID-19 had lower odds of being current smokers than patients admitted with other respiratory viruses (ORadj=0.55, 95% CI=0.31-0.96, p=.04). Odds were equivocal for former smokers (ORadj=1.08, 95% CI=0.72-1.65, p=.70). Current smoking in cases was significantly lower than expected from London prevalence (9.4% vs. 12.9%, p=.02). Smoking status recorded on the EHR deviated significantly from that recorded within the medical notes (χ2(3)=226.7, p<.001).
Interpretation In a single hospital trust in the UK, patients hospitalised with COVID-19 had reduced odds of being current smokers compared with patients admitted with other respiratory viruses a year previous.
Funding UK BBSRC, Cancer Research UK, UKPRP.
INTRODUCTION
COVID-19 is a respiratory disease caused by the SARS-CoV-2 virus. There are in excess of 50 million confirmed COVID-19 cases globally, with over one million deaths reported[1]. Large age and sex differences in case severity and mortality have been observed[2], with hypertension, diabetes and obesity identified as important risk factors[3]. There are a priori reasons to believe that current smokers are at increased risk of contracting COVID-19 and experiencing greater disease severity once infected. SARS-CoV-2 enters epithelial cells through the ACE-2 receptor[4]. Evidence suggests that gene expression and subsequent ACE-2 receptor levels are elevated in the airway and oral epithelium of current smokers[5, 6], potentially making smokers vulnerable to contracting SARS-CoV-2. The regular hand-to-mouth movements involved in cigarette smoking may also increase SARS-CoV-2 transmission. Other studies, however, show that smoking downregulates the ACE-2 receptor[7]. These uncertainties notwithstanding, both former and current smoking increase the risk of other respiratory viral[8] and bacterial[9] infections and are associated with worse outcomes once infected. For example, a large observational study in the UK found that former and current smokers had increased odds of being hospitalised with community-acquired pneumonia compared with never smokers[10]. However, early data from the ongoing pandemic have not provided clear evidence for an independent association of smoking status with COVID-19 outcomes[11, 12].
A living evidence review of observational and experimental studies examining the association of smoking status with COVID-19 infection, hospitalisation, disease severity and mortality has found that, among 279 studies, current smoking (not adjusted for age, sex or comorbidities) was generally lower than what would be expected from national smoking prevalence[12]. In addition, current smokers were at reduced risk of testing positive for SARS-CoV-2 compared with never smokers, and former smokers were at increased risk of hospitalisation, disease severity and in-hospital mortality compared with never smokers. However, the majority of included studies were limited by the lack of appropriate controls, poor recording of smoking status and insufficient adjustment for relevant covariates. Many studies relied on routine electronic health records (EHRs) to obtain individual-level data on demographic characteristics, comorbidities and smoking status. Previous research suggests that data on smoking status obtained via EHRs tend to be incomplete or outright inaccurate, with implausible longitudinal changes observed[13]. In addition, as hospitalised populations differ by age and sex from the general population, comparisons of current and former smoking prevalence in hospitalised and non-hospitalised populations are likely limited. There is hence an urgent need for alternative study designs with relevant comparator groups (e.g. populations hospitalised with a similar type of respiratory viral infection) and adjustment for covariates to better understand the association of smoking status with COVID-19 disease outcomes.
We therefore aimed to i) examine, in a retrospective case-control study conducted at a single UK hospital trust, the association of smoking status with hospitalisation for COVID-19 compared with hospitalisation for other respiratory virus infections (e.g. influenza, respiratory syncytial virus) a year previous; ii) compare current smoking prevalence in the case population with age- and sex-matched London prevalence, with estimates obtained from the nationally representative Annual Population Survey; and iii) examine whether there is discordance between smoking status recorded on the summary EHR and within the contemporaneous medical notes.
METHODS
Study design
This was an observational, retrospective, case-control study performed at a single National Health Service (NHS) hospital trust (comprising two hospital sites) in London, UK. The study protocol and analysis plan were pre-registered on the Open Science Framework (https://bit.ly/3kFYh06). The pre-registered protocol stipulated a non-inferiority design (i.e. a one-tailed statistical test) to maximise statistical power to detect a significantly lower proportion of current smokers among patients hospitalised with COVID-19 compared with patients hospitalised with another respiratory viral infection a year previous. The protocol was amended after data collection but prior to statistical analysis (https://osf.io/ezfqs/) to implement a traditional case-control design (i.e. a two-tailed statistical test), as a delay in study approval meant that the number of eligible cases and controls exceeded our expectations. Hence, the obtained sample size was deemed sufficient for a two-tailed test. A completed STROBE checklist is available in the additional file. This amended study was designed to test the hypothesis that current smoking is underrepresented in patients hospitalised with COVID-19 compared with those hospitalised with other respiratory viruses a year previous. Ethical approval was obtained from a local research committee and the NHS Health Research Authority (IRAS_282704). The requirement for informed consent was waived due to the nature of the study.
For comparison, aggregated data on current, former and never smoking prevalence for London was obtained from the Office for National Statistics (ONS) Annual Population Survey[14].
A sample size calculation, updated after data collection but prior to data analysis (https://osf.io/ezfqs/), indicated that 363 cases and 109 controls would provide 80% power to detect a 10% reduction in current smoking prevalence in cases compared with controls (i.e. 10% in cases and 20% in controls) with alpha set to 5%. We included all cases from 1st March 2020 to the 26th August 2020 (the date on which data were obtained) and all controls from the 1st January 2019 and the 31st December 2019.
Eligibility criteria
Inclusion criteria
Cases
Consecutive patients admitted to an adult hospital ward (i.e. 18+ years) between 1st March 2020 and 26th August 2020 (the date on which data were obtained);
Diagnosis of COVID-19 on or within 5 days of hospital admission, identified via associated International Classification of Diseases version 10 (ICD-10) codes[15]. This temporal boundary was set to prevent inclusion of patents with nosocomial (hospital-acquired) infection and allowed for a delay of 3 days in requesting a COVID-19 test and 2 days for receiving and reporting the results on the EHR. The median incubation time for COVID-19 is estimated at 5.1 days (95% CI = 4.5-5.8)[16]. We sought to exclude individuals with nosocomial COVID-19 infection as they are a different population (e.g. older, more frail) compared with those infected in the community and subsequently requiring hospitalisation.
Controls
Consecutive patients admitted to an adult hospital ward (i.e. 18+ years) between 1st January 2019 and 31st December 2019;
Diagnosis of a viral respiratory infection (e.g. influenza, parainfluenza) on or within 5 days of admission, identified via ICD-10 codes. Patients hospitalised with respiratory viruses other than COVID-19 were deemed appropriate controls due to the similar mechanism for transmission (i.e. respiratory droplets and aerosols)[17]. In addition, risk factors for hospitalisation with other respiratory viruses are similar to those for hospitalisation with COVID-19 (e.g. age, comorbidities)[18, 19].
Exclusion criteria
Cases and controls
No record of smoking status on the summary EHR or within the medical notes;
A primary diagnosis of infectious exacerbation of COPD due to the strong causal association of COPD with current and former smoking.
Measures
Data on demographic and smoking characteristics were collected from the summary EHR or the medical notes. In the UK, the summary EHR is produced at the point of an individual’s first interaction with a specific NHS hospital trust. Further information is added to the summary EHR following subsequent interactions with the hospital trust. The medical notes include contemporaneous clinical notes, General Practitioner referral letters and outpatient clinic letters, and are updated more frequently than the summary EHR.
Outcome variable
The outcome of interest was the type of hospital admission (i.e. with COVID-19 vs. other respiratory viral infections).
Exposure variable
Smoking status (i.e. current, former, never) was obtained from the summary EHR or the medical notes. A number of cases were recorded as ‘non-smokers’ without distinguishing between ‘former smokers’ and ‘never smokers’. For the primary analysis, patients categorised as a ‘non-smoker’ were treated as ‘never smokers’. Where possible, information on use of smokeless tobacco, waterpipe and/or alternative nicotine products (e.g. e-cigarettes) was extracted. The joint first authors searched within the contemporaneous medical records for free-text entries of smoking status. The most recently available record of smoking status, obtained from either the summary EHR or the medical notes, was extracted. Where available, data on pack-year history of smoking were extracted.
Covariates
Covariates included age, sex, ethnicity, socioeconomic position (with post codes linked by the research team to the Index of Multiple Deprivation (IMD)[20]) and comorbidities (classified by organ system, including cardiac, metabolic and respiratory diseases). Medical conditions not expected to be strongly associated with COVID-19 hospitalisation were not considered in the analyses (e.g. sciatica and fibromyalgia; see the additional file). Age was treated as a continuous variable in the primary analysis, with banded age groups (i.e. 18-29 years, 30-44 years, 45-59 years, 60-74 years, 75-89 years and > 90 years) used in exploratory analyses. The IMD was categorised as quintiles to reduce the impact of sparse data.
Data analysis
All analyses were conducted in R version 4.0.2.[21] Descriptive statistics for cases and controls are reported. To explore differences between cases and controls, Pearson’s Chi-square tests, Cochran-Armitage tests for trend and ANOVAs were used, as appropriate.
To examine the association of former and current smoking with hospitalisation for COVID-19 compared with hospitalisation for other respiratory virus infections, unadjusted and adjusted generalised linear models with a binomial distribution and logit link function were performed. We report odds ratios (ORs), 95% confidence intervals (CIs) and p-values. Two sensitivity analyses were performed. First, those recorded as ‘non-smokers’ were removed from the analysis. Second, those excluded from the analytic sample due to missing data on smoking status (see section above on ‘Exclusion criteria’) were included and coded as i) ‘never smokers’ and then as ii) ‘current smokers’.
We then compared age-stratified current smoking prevalence in the case population with overall London prevalence stratified by age and weighted by the sex distribution of the case population.
To examine the concordance between smoking status recorded on the summary EHR and within the contemporaneous medical notes, Pearson’s Chi-squared tests were performed for the entire sample, and then separately for cases and controls.
RESULTS
A total of 610 potential cases and 514 potential controls were identified. A total of 446 cases and 211 controls were included in the analytic sample (see Figure 1). Thirteen potential controls and 60 potential cases were excluded due to not having a record of documented smoking status. This was likely due to these patients having no prior contact with the selected NHS foundation trust. Notably, 37 (62%) of potential cases that were excluded because of missing smoking status did not survive to hospital discharge, with no in-hospital mortality in potential controls, which suggests that data were not missing at random.
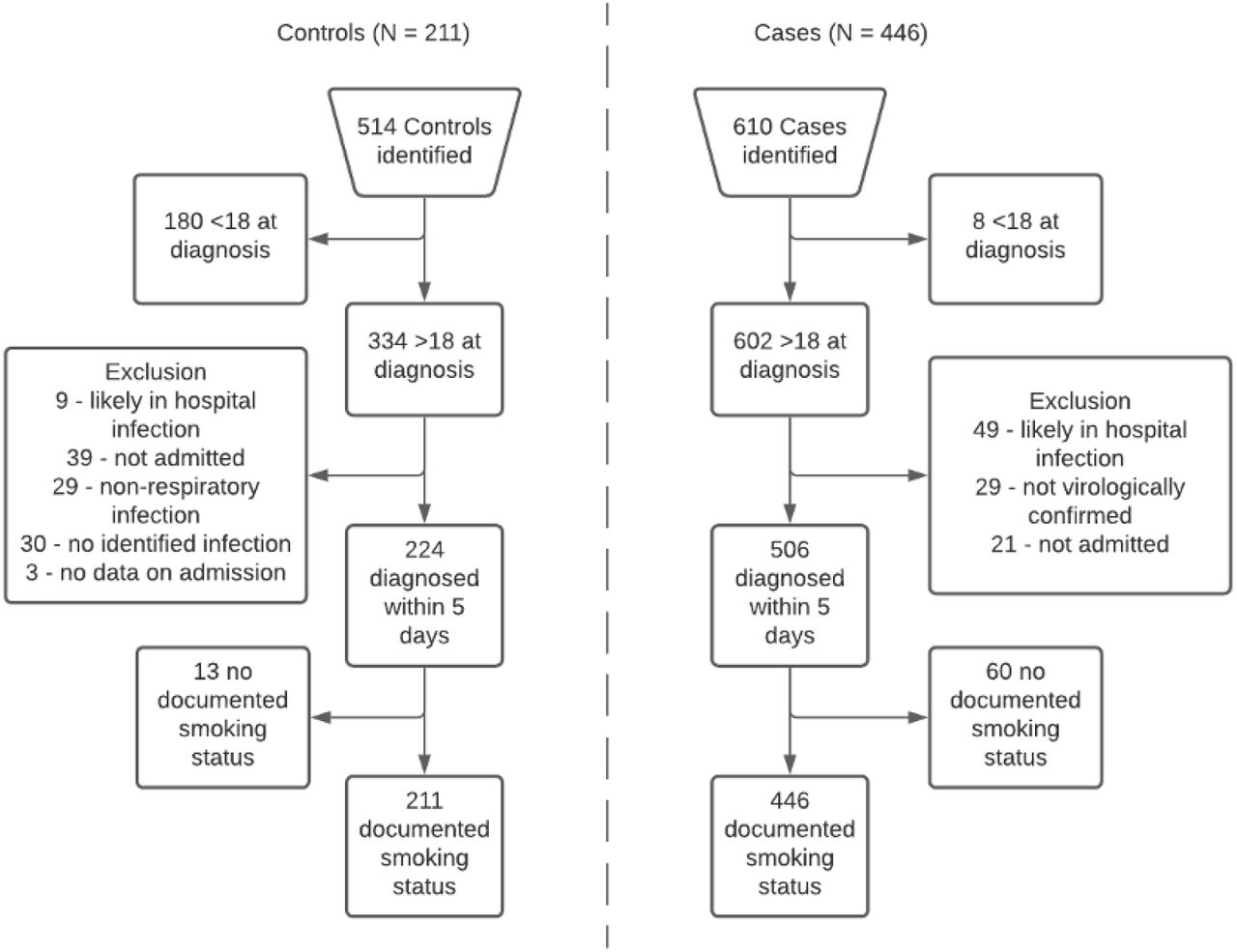
Eligibility flow diagram for controls (left hand side) and cases (right hand side).
Compared with controls, cases were more likely to be male (55% vs. 35.9%) and older (64.9 years vs 62.5 years) (see Table 1). Approximately 10% of cases and controls had missing data for ethnicity. Compared with cases, controls were more likely to be admitted from more deprived areas (IMD quintiles 1 and 2) (41.8% vs. 32.9%, p < 0.001) and have pre-existing metabolic (30.3% vs 13.3%) and cardiac comorbidities (53.4% vs 30.3%). A significantly larger proportion of cases compared with controls did not survive to discharge (28.7% vs. 4.3%). Among 128 cases not surviving to discharge, 53 (41.4%) were never smokers, 63 (49.2%) were former smokers and 12 (9.4%) were current smokers. For patients who survived to discharge, the median length of hospital stay for cases and controls was 9 (IQR = 4-18) and 4 (IQR = 2-9) days, respectively (see Table 1).
Demographic and smoking characteristics of cases and controls.
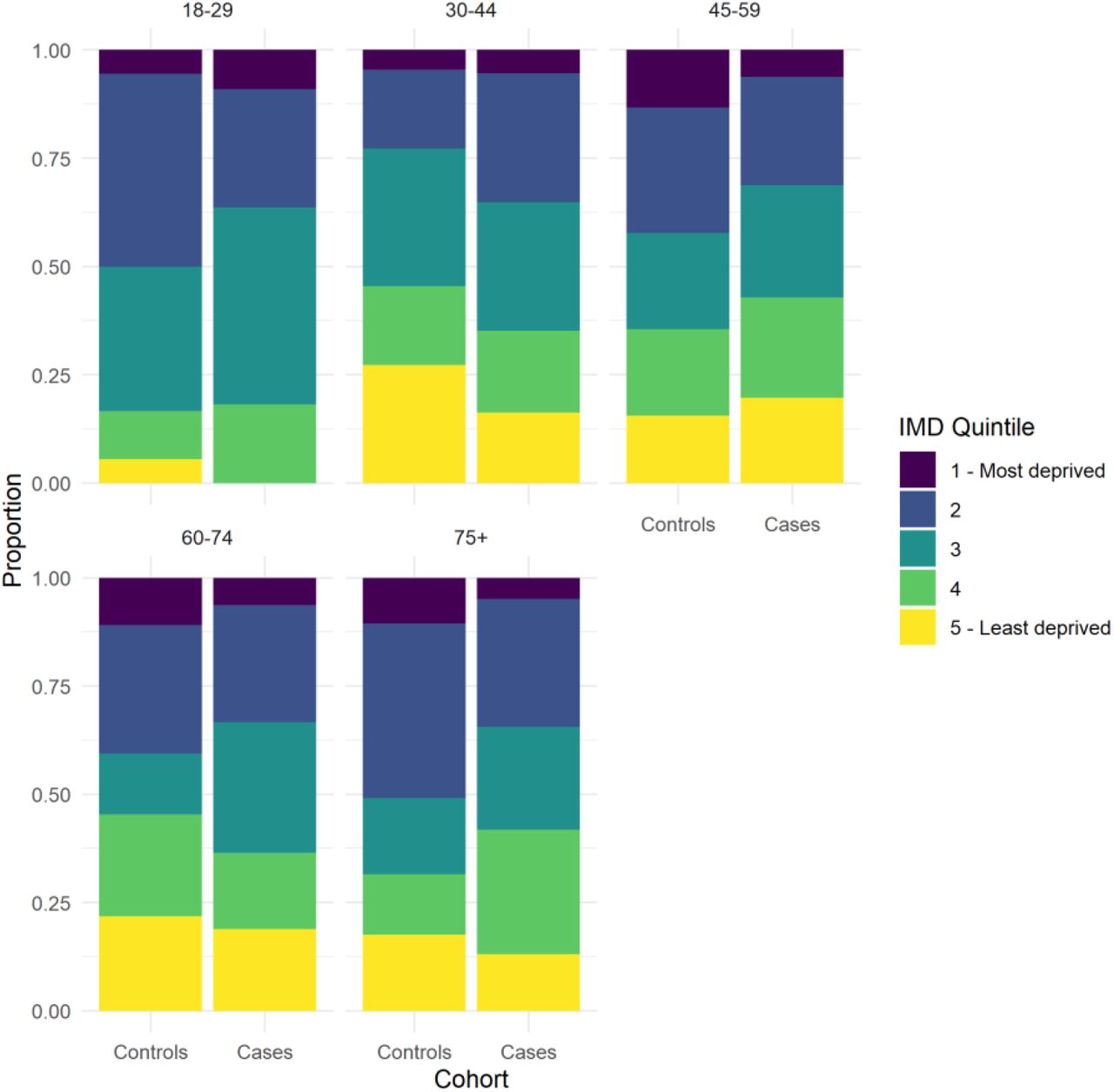
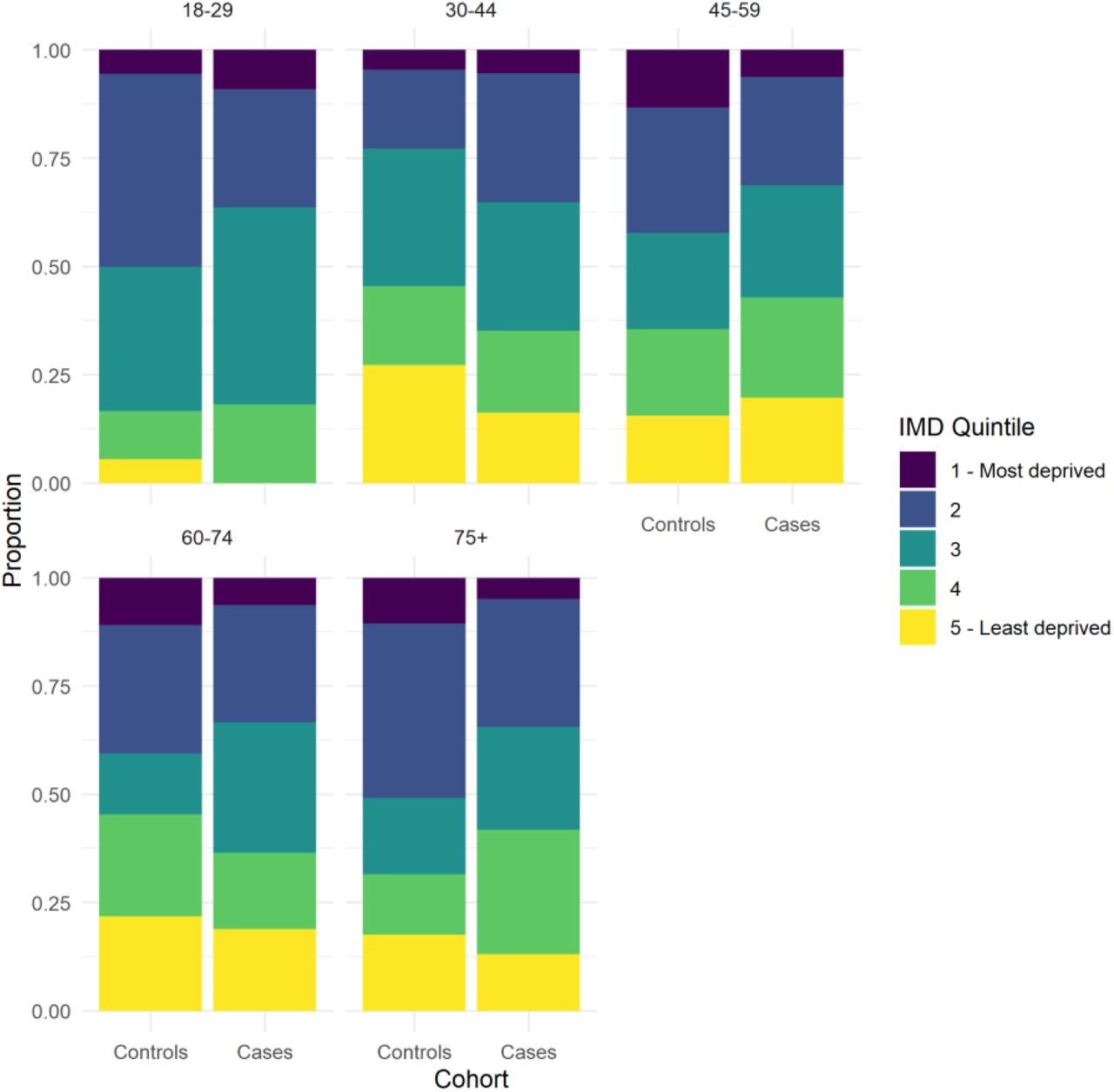
Cases and controls were predominantly admitted from North central and North East central London (see additional file figure 1). The number of cases admitted from peripheral locations was greater than in controls and represents transfer of inpatients from other hospitals and diversion of patients that would otherwise have attended local hospitals due to bed pressures. The Chi-square test for trend found inconclusive evidence for any difference in socioeconomic position between cases and controls, χ2(3) = 8.93, p = 0.06 (see additional file figure 2).

Concordance between smoking status recorded on the summary EHR and the medical notes for controls (red) and cases (blue).
Association of smoking status with type of hospitalisation
The prevalence of former smoking was higher in cases compared with controls (38.6% vs. 31.8%). Current smoking prevalence was lower in cases compared with controls (9.4% vs. 17.1%). A single patient from the case cohort was recorded as a dual cigarette and e-cigarette user. Two patients, one from each cohort, were recorded as dual cigarette and shisha/waterpipe users. Pack-year history of smoking was only recorded for 40% of patients with a smoking history (see Table 1).
In the univariable analysis, patients hospitalised with COVID-19 had reduced odds of being a current smoker compared with those admitted with other respiratory viruses (OR = 0.52, 95% CI = 0.31-0.86, p = 0.01). The odds for former smokers were equivocal (OR = 1.16, 95% CI = 0.81-1.68, p = 0.43).
In the multivariable analysis adjusted for sex, age, socioeconomic position and comorbidities, patients hospitalised with COVID-19 had reduced odds of being a current smoker compared with those admitted with other respiratory viruses (OR = 0.55, 95% CI = 0.31-0.96, p = 0.04). The odds for former smokers were equivocal (OR = 1.08, 95% C.I. = 0.72-1.61, p = 0.70).
Sensitivity analyses
First, in a sensitivity analysis with patients recorded as ‘non-smokers’ excluded from the sample (leaving 398 cases and 159 controls), patients hospitalised with COVID-19 had reduced odds of being a current smoker compared with those admitted with other respiratory viruses (OR = 0.41, 95% CI = 0.22-0.74, p = 0.03). The odds for former smokers were equivocal (OR = 0.78, 95% C.I. = 0.49-1.23, p = 0.28).
Second, in a sensitivity analysis with those with missing data on smoking status (n = 73) treated as ‘never smokers’ (resulting in 506 cases and 224 controls), patients hospitalised with COVID-19 had reduced odds of being a current smoker compared with those admitted with other respiratory viruses (OR = 0.51, 95% CI = 0.30-0.88, p = 0.01). Next, when those with missing data on smoking status were treated as ‘current smokers’, patients hospitalised with COVID-19 had equivocal odds of being a current smoker compared with those admitted with other respiratory viruses (OR = 0.94, 95% CI = 0.61-1.46, p = 0.80).
Comparison with London smoking prevalence
Compared with age-stratified London prevalence weighted by sex, similar current smoking prevalence in cases were observed in the 30-44 years, 60-74 years and 75+ years age groups (see Table 2). Current smokers were overrepresented in the 18-29 years age group and underrepresented in the 45-59 years age group. Former smokers were consistently overrepresented in cases compared with age-stratified London prevalence weighted by sex, except for those aged 18-29 years.
Smoking prevalence in cases and controls compared with London prevalence.
Concordance of smoking status recorded on the summary EHR and the medical notes
Controls were more likely to have no record of smoking status on the summary EHR compared with cases (75.4% vs. 7%) (see Figure 2). Smoking status on the summary EHR was incorrectly recorded for 168 controls and 60 cases (χ2(3) = 226.7, p = < 0.001). In cases, six current smokers were misclassified as former smokers, one current smoker as a never smoker and six current smokers had no record of smoking status on the summary EHR. In controls, six current smokers were misclassified as former smokers and 23 current smokers had no record of smoking status on the summary EHR. There was greater discordance between smoking status recorded on the summary EHR and within the medical notes in controls (χ2(3) = 256.5, p = < 0.001) than in cases (χ2(3) = 34.2, p = < 0.001).
DISCUSSION
This observational, retrospective, case-control study with patients admitted to a single UK hospital trust found a lower proportion of current smokers in cases hospitalised with COVID-19 during the first phase of the pandemic compared with controls hospitalised with other respiratory viral infections a year previous. The observed reduction in current smoking prevalence was robust to adjustment for sex, age, socioeconomic position and comorbidities. The low prevalence of current smoking in cases appeared driven by current smokers being underrepresented in those aged 45-59 years, with similar to expected current smoking prevalence in the other age groups. It should be noted that cases aged 45-59 years were more likely to reside in less deprived areas than controls. As smoking status is strongly associated with socioeconomic position[14], this may partly explain the lower smoking prevalence in this age group.
Further, we found that smoking status is typically poorly recorded in the summary EHR. This was more prominent in controls than cases – a difference that is likely explained by the observation that COVID-19 patients were followed up by the respiratory medicine team after discharge as part of a COVID-19 follow-up clinic where they specifically asked about smoking status[22]. The observed discrepancy between smoking status recorded on summary EHRs and the contemporaneous medical notes is a concern, particularly for studies relying solely on EHRs as the source of information on smoking status.
Strengths and limitations
To our knowledge, this is one of few studies specifically designed to examine the association between smoking status and hospitalisation with COVID-19. It was further strengthened by the inclusion of a control population hospitalised with other respiratory viruses, a comparison with local smoking prevalence derived from a nationally representative survey and an assessment of the quality of data on smoking status gleaned from summary EHRs.
This study also had a number of limitations. First, current smoking is expected a priori to be associated with hospitalisation for non-COVID-19 respiratory viruses[23]. Hence, the use of this control population may have biased towards the null any association between smoking status and type of hospitalisation due to greater smoking prevalence in controls compared with the general population at risk of COVID-19[24]. To minimise any impact of this on the interpretation of results, we included a community-level comparator of overall London smoking prevalence. Second, the IMD was used to capture the socioeconomic position of patients, calculated for a spatial boundary referred to as a Lower Layer Super Output Area[20], which are geographic areas of populations of ∼1500 individuals, which can then be linked to post codes. In densely populated and socioeconomically diverse areas such as central London, the ability of the IMD to capture socioeconomic position may be limited[25]. Third, the control population was selected to reflect commonalities in the transmission of respiratory viruses. However, emerging evidence suggests that COVID-19 has a significantly different pathological process compared with other respiratory viruses. For example, mortality rates from COVID-19 differ widely from those due to epidemic influenza[26]. Further, mortality rates for COVID-19 differ between and within countries and over the course of the pandemic, at least partly due to improving knowledge and treatment of the disease[27]. In addition, the risk of superadded bacterial infection in COVID-19 patients appears lower than for those with influenza[28]] and COVID-19 patients have increased rates of coagulopathies compared with other respiratory viruses[29]. Taken together, these emerging observations may limit any direct comparison of risk profiles in cases and controls. Fourth, a history of current or past cancer was high in both groups at greater than 20% and was significantly greater in controls compared with cases. This reflects a bias in the population that regularly interacts with the selected NHS hospital trust, which is a specialist cancer referral centre. We visualised the geographic regions where patients were admitted from to examine any systemic differences between cases and controls, and caution that the differing catchment areas of the two cohorts may have led to important differences in the underlying populations. In addition, during the peak of the first wave of the pandemic in the UK, many cases were transferred across hospital sites due to bed pressures.
Implications for policy and practice
COVID-19 will continue to place a large burden on healthcare services in the UK and internationally over the coming months and years. To mitigate against this, multiple non-pharmacological interventions are being implemented to reduce the intensity of demand on acute and intensive services. Irrespective of any direct link between smoking and COVID-19 disease outcomes, smoking is a significant cause for healthcare demand globally. We have argued elsewhere for the need to ramp up smoking cessation support to reduce the current and future burden on healthcare and social services[30].
Avenues for future research
To better understand the role of smoking as a risk factor for COVID-19 hospitalisation, longitudinal, representative population-level studies from multiple sites are required. A large, multinational clinical cohort study (the International Severe Acute Respiratory and emerging Infection Consortium; ISARIC) collects smoking status but this is likely obtained from summary EHRs. Purposeful acquisition of accurate smoking status is required to characterise the role of smoking in COVID-19 disease outcomes.
Conclusion
In a single hospital trust in the UK, patients hospitalised with COVID-19 had reduced odds of being current smokers compared with patients admitted with other respiratory viruses a year previous. In the 45-59 year age group, lower smoking prevalence than would be expected based on age- and sex-matched local smoking prevalence was observed. Smoking status was poorly recorded, with high observed discordance between smoking status recorded on the summary EHR and the medical notes.
Data Availability
Anonymised and de-identified individual-level data are available upon request and approval from the NHS foundation trust. Requests should be directed to the corresponding author. Alternatively, data can be requested directly from the Biomedical Research Centre Clinical and Research Informatics Unit at UCL/UCLH.
DATA SHARING
Anonymised and de-identified individual-level data are available upon request and approval from the NHS foundation trust. Requests should be directed to the corresponding author. Alternatively, data can be requested directly from the Biomedical Research Centre Clinical and Research Informatics Unit at UCL/UCLH.
CONTRIBUTERS
DS, OP, LS, JB and RB conceived of and designed the study. DS and RB acquired the study data. DS and OP extracted and analysed the data. DS, OP, LS, JB contributed to the interpretation of the data and to the drafting of the manuscript. All authors have read and approved the manuscript.
DECLARATION OF INTERESTS
DS, OP and RB have no conflicts of interest to declare. LS has received a research grant and honoraria for a talk and travel expenses from manufacturers of smoking cessation medications (Pfizer and Johnson & Johnson). JB has received unrestricted research funding to study smoking cessation from companies who manufacture smoking cessation medications. All authors declare no financial links with tobacco companies or e-cigarette manufacturers or their representatives.
ROLE OF FUNDERS
We gratefully acknowledge all funding listed above. The views expressed are those of the authors and not necessarily those of the funders.
ETHICAL APPROVAL
Ethical approval was obtained from a local research committee and the NHS Health Research Authority (IRAS_282704). The requirement for informed consent was waived due to the nature of the study.
Additional File

Primary location of residence of controls (L) and cases (R) enrolled in the study. The location of the study site is marked by a black dot. n.b. visualised region is limited to central London.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
IMD quintile for admitted controls and cases for each age group.
Weightings matching London APS data to case population
ICD-10 code list
Cases
U07.1 - COVID-19, virus identified
Controls
J10.1 - Influenza with other respiratory manifestations, seasonal influenza virus identified
J10.0 - Influenza with pneumonia, seasonal influenza virus identified
J11.0 - Influenza with pneumonia, virus not identified
J12.2 - Parainfluenza virus pneumonia
J12.0 - Adenoviral pneumonia
J10.8 - Influenza with other manifestations, seasonal influenza virus identified
J11.1 - Influenza with other respiratory manifestations, virus not identified
J12.8 - Other viral pneumonia
J12.9 - Viral pneumonia, unspecified
J12.3 - Human metapneumovirus
J20.8 - Acute bronchitis due to other specified organisms
J21.8 - Acute bronchiolitis due to other specified organisms
Comorbidity code list
Auto-immune
Myasthenia gravis
Systemic Lupus Erythematosus
Crohn’s
disease
Ulcerative colitis
Granulomatosis with Polyangiitis
Sjogren’s syndrome
Cold agglutinin disease
Grave’s disease
Rheumatoid arthritis
Cancers
All cancers
All carcinomas
All myelodysplasias
Waldenstrom’s macroglobulinaemia
All myelomas
All lymphomas
All leukaemias
Gliomas
Sarcomas
Melanomas
Cardiac
Hypertension
Ischaemic heart disease
Coronary artery disease
Atrial fibrillation
Congestive cardiac failure
All other heart failure
Non-ST elevation myocardial infarction
Myocarditis
History of coronary artery bypass graft
Aortic stenosis
Other valvular abnormalities
Presence of a pacemaker/implantable cardiac defibrillator
All cardiomyopathies
Structural cardiac abnormalities
Haematological
Sickle cell disease
All thalassaemias
Thrombotic thombocytopenia purpura
Anaemia
Metabolic
Obesity
Type-1 Diabetes Mellitus
Type-2 Diabetes Mellitues
Syndrome of inappropriate ADH
Hypothyroidism
Addison’s disease
Pituitary hormone abnormalities
Chronic pancreatitis
Neurological
History of acute stroke
Parkinson’s disease
History of transient ischaemic attack
Multiple sclerosis
Epilepsy
Cerebral Palsy
All dementias
Autism
Ataxic disorders
No relevant comorbidities
Nil
Alcohol excess
Achalasia
Sciatica
Substance misuse
Benign prostatic hypertrophy
Psychiatric
Schizophrenic disorders
Anorexia nervosa
Renal
Chronic kidney disease
History of acute kidney disease
Renal transplant
Respiratory
Obstructive sleep apnoea
Pulmonary hypertension
Chronic obstructive pulmonary disease
Asthma
Pulmonary fibrosis
Bronchiectasis
Interstitial lung disease
Emphysema
History of or current tuberculosis
Sarcoidosis
History of pulmonary embolus
ACKNOWLEDGEMENTS
DS is supported by a PhD studentship from the UK Biotechnology and Biological Sciences Research Council [BB/M009513/1]. OP receives salary support from Cancer Research UK (C1417/A22962). JB, LS, & OP are members of SPECTRUM, a UK Prevention Research Partnership Consortium (MR/S037519/1). UKPRP is an initiative funded by the UK Research and Innovation Councils, the Department of Health and Social Care (England) and the UK devolved administrations, and leading health research charities.
REFERENCES




