
ABSTRACT
The effect of Zinc (Zn) sufficiency/supplementation of the populations on the occurrence of COVID-19 and associated severe illness/mortality remains unknown. Worldwide, general recommendations for Zn sufficiency and immune-boosting for COVID-19 are in place. A time-series association study was conducted on 23 different Zn sufficiency level but socially similar European populations/countries (Population: 522.47million; experiencing up to >150 fold difference in death rates) with supposedly similar confounders and stage of the pandemic, covering the period from pre-peak-of-infections to post-peak-of-infections till flattening of the 1st wave of infections (12 March to 26 June). Comparison of these populations, consistently displayed a strong and significant correlation/covariation of populations’ Zn sufficiency/supplementation status with the COVID-19 mortality [Pearson’s r(23): 0.7893–0.6849, p-value<0.0003] and cases per million [r(23):0.8084 to 0.5658; p-value<0.005], without requiring adjustments or extra exclusion/inclusion criterion being applied elsewhere, e.g., age, age distribution, comorbidities, sex, urbanization. Among the analyzed countries, elevated 9X mortality risk was observed for populations with >92.5 % Zn sufficiency levels at all times as compared to populations with lower Zn sufficiency. The presence of a small percentage of adults/elderly with conditions/comorbidities in the populations susceptible to higher Zn intake/supplementation related pathologies (Prasad et al., JAMA.1978; 240(20):2166-2168) could be suspected for the paradoxical observation. Controlled trials or retrospective analysis of the adverse event patients’ data seem warranted for ascertaining the basis of the observation in uncertain terms for allowing the harnessing of the full protective potential of the Zn supplementation for populations.
INTRODUCTION
The epidemiological data exploring the role of Zinc (Zn) sufficiency of the population on SARS-CoV-2 caused COVID-19 disease are practically nonexistent. It is a key micronutrient known to play important role in immune competence and wellbeing (1). The explicit and implicit general recommendation for immune augmentation of population and COVID-19 patients by healthy diet or supplementation is in place for its potential protective role in infections and other immune and oxidative stress-related conditions/pathologies relevant to COVID-19 (2). Globally, Zn deficiency among populations ranges from 3-50% (3). The developed European and North American nations generally have the most sufficiency while African and Asian nations the least. Its deficiency in populations is widely associated with vulnerability to infectious diseases, chronic immune system disorders, and medical conditions (1-4).
The Zn levels are tightly regulated in the human body and its differential levels are maintained in various organs, tissues, and extracellular milieu including serum through complex homeostasis mechanism. Though not always appropriate serum levels are generally considered as reflective of Zn deficiency/sufficiency in the absence of more accurate measures and usually in combination with overt pathological features are used to diagnose pathological deficiency and subsequent recommendation/prescription of Zn supplementation or augmentation of its levels through diet modifications but not always without adverse outcome or failures in certain conditions more common in elderly and relevant to COVID-19 adverse events, e.g., sickle cell disease, chronic kidney diseases (4,5).
The current epidemiological time-series analysis assessed the association of Zn sufficiency of populations with COVID-19 mortality, testing the null-hypothesis that Zn sufficiency/levels are not associated with COVID-19 mortality in populations.
RESULTS
Globally COVID-19 mortality rates positively covary with Zinc sufficiency levels
Zinc sufficiency/deficiency levels vary across the globe (Supp. Fig. 1A). Differential COVID-19 mortality rates had been observed among countries with European and North American countries with higher HAQ Index, Life expectancy, Median age (6,7) being the worst affected (Sup. Fig. 1B-C). Trained-immunity (8,9), BCG vaccination (10), vitamin D (11), Zinc deficiency (12) had been previously associated with reduced COVID-19 mortality using early-stage pandemic data (8-12), though not without controversies for inclusion/exclusion criteria, non-matched pandemic stages, appropriateness of the data set and loss of association with the time post-peak-of-infections (8,9,11,13). The COVID-19 mortality rate in socially similar populations (Boxed NA and EU) is strongly associated with their Zinc sufficiency (Sup. Fig. 1A; time-series graphics available at ref. 7). European, North American and South American countries reporting high mortality have been the high Zinc sufficiency countries. Globally the populations were exposed to COVID-19 at different time-points, had differential access to medical facilities, life-style, social-structure, preventive measures in place, supposed associations drawn from them could be tenuous due to disparate data sets. Therefore, pandemic phase-matched (Sup. Fig. 2 A-B), socially similar European populations with comparable confounders (8,10,11,13) were analyzed to arrive at more dependable conclusions.
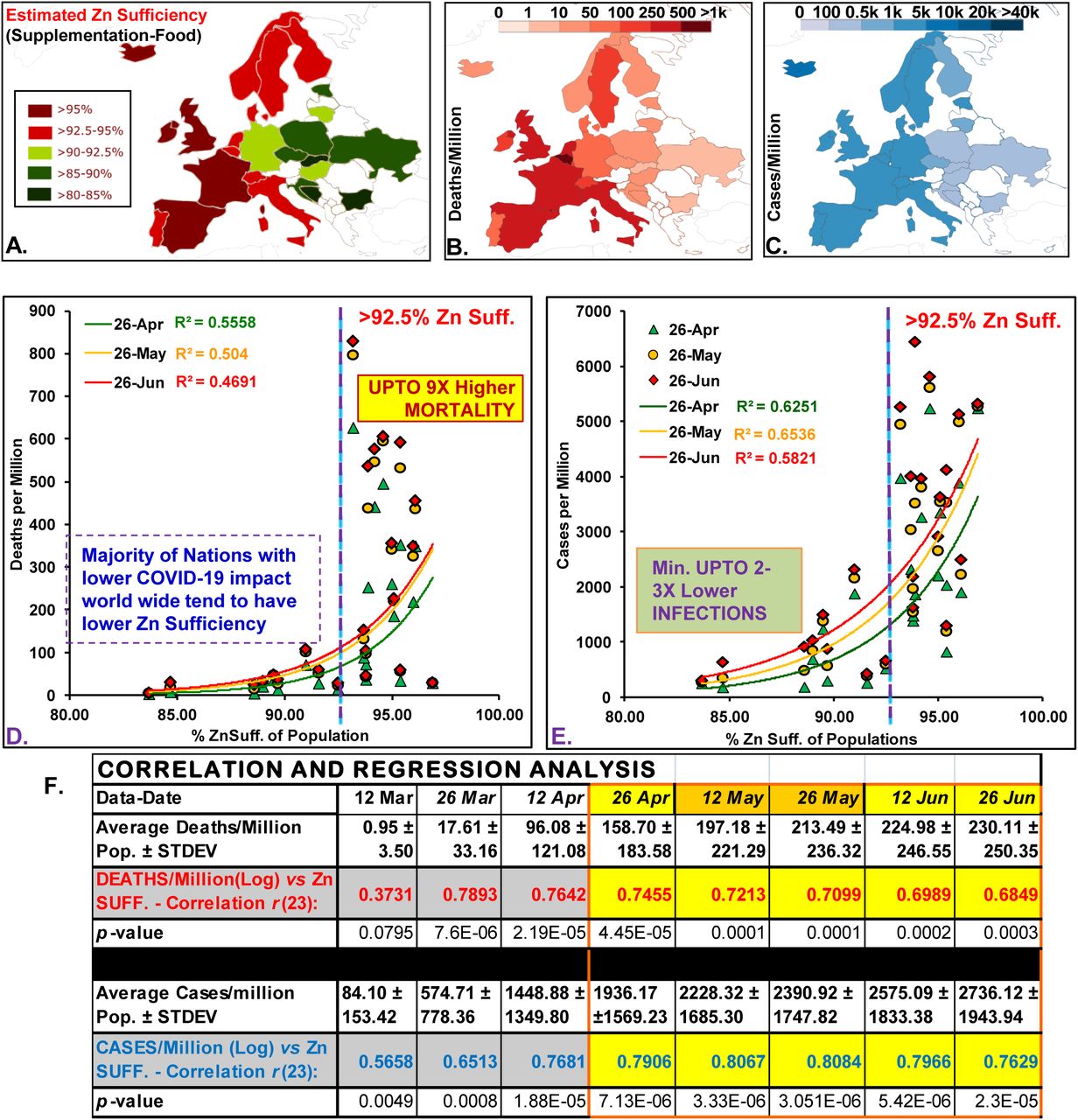
Study populations: (A) Zn sufficiency estimates, and (C) deaths and cases/million (26th April). Deaths (D) and cases (E) per million population positively correlated with their Zn sufficiency levels. (F) Correlation analysis for the most synchronized period of infections and response (highlighted yellow–covers the rise and flattening of infections/mortality rate (see Supp. Fig. 1)

{kind=link}
{kind=link}
(A) High suff. countries (n=12) consistently had higher CFR than low Zn suff. Countries (n=11). For both group of countries CFR is on a downward trend over-time post-infections-peak. (B) High Zn suff./supplementation countries consistently reported higher infections than Low Zn suff. Countries#. The differential gap is slowly closing over time as expected with pandemic progression. Note: fold difference in mortality rates would exponentially increase with Zn Suff. cutoff of values used.
Analysis of socially similar countries
Zinc sufficiency strongly and significantly correlated with COVID-19 mortality
The Zinc sufficiency in socially similar 23 European populations (Fig 1A, Supp. Table 1) positively associated with COVID-19 mortality and infection rates (Fig. 1B-C). The mortality and infections covaried exponentially with Zn sufficiency (Fig. 1D-E). Above >92.5% Zn sufficiency, the populations experienced upto 9X higher deaths (Fig. 1D). Pearson’s correlation for the most synchronized period of infections and response (26 April to 26 June, Supp. Fig. 2) was strong [Fig. 1F, Deaths per million: r(23)= 0.7455–0.6849, p<0.0003; Cases per million: r(23)= 0.8084–0.7629, p<0.00002]. Even the division of countries using >93.7% sufficiency cutoff, indicated high mortality (5.79 to 2.66X) and incidences (4.5-2.3 fold) in High Zn sufficiency populations (n=12) as compared to Low sufficiency (n=11).
Higher Zn sufficiency populations consistently reported higher case fatality rates (CFRs) and incidence rates
The CFRs of different sufficiency population groups, i.e., high (>93.7%, 12 countries) vs low (<93.7% 11 countries) had been essentially different and showing decline post-peak-of-infections, i.e, 12 May (Fig. 2A) possibly indicative of an increase in protected population but the relative change in the CFR decrease had been lower for the higher sufficiency countries and the gap had been consistently increasing (about 16% on 26 June) (Fig. 2B).
DISCUSSION
General positive correlation of COVID-19 mortality and cases with Zn sufficiency levels was observed, which sustained till the flattening of the curves. Nevertheless, comparison of socially similar’ populations/countries at similar phase/stages of the pandemic with comparable potential confounders, closely graded Zn sufficiency, globally accounting for 34.2% mortality (173 thousand deaths) gives confidence to observations made. However, the use of Zn sufficiency estimates from 2005, in the absence of any recent data, as a surrogate for the current levels in populations may somewhat limit our degree of confidence in the analysis. For the sake of current analysis and discussion, it may be assumed that drastic overall changes in Zn sufficiency levels may have not taken place, except the expected Zn sufficiency improvement with the development index and the availability of diverse foods and supplements. The surprisingly strong association between Zn sufficiency of populations with COVID-19 mortality and incidences for the whole study duration even stronger than those being hotly discussed, debated, and evaluated in clinical trials [10,11,13], warrants thorough endeavors to reap the benefits of Zn supplementation by the populations without endangering few.
Though the variable responsible for the observed association remains unknown, we may conjure that the increased mortality observed in high Zn sufficiency populations could be contributed by the existing certain small percentage of populations with underlying conditions as a result of altered genetic composition, physiology, response to Zn supplementations/modulation [4,5] making them prone to display characteristic COVID-19 adverse illness as a result of increased oxygen radical generation or compromised diminished oxidative stress handling system due to their physiologies propensity to promote the pro-oxidant role of Zn on supplementation [14]. Here it may be indicated that the Zn overdose may not be uncommon in the highly impacted general aged population of the developed countries that are more receptive to supplementation with or without a prescription [15].
In conclusion, the observations presented underscore the need to undertake exploratory studies to identify and link underlying conditions that could make certain ‘supposed’ Zn sufficient individuals prone to COVID-19 mortality. The outcomes could help devise a better more thorough molecular evidence-based comprehensive Zn supplementation based immune augmentation management and control practices for COVID-19 control.
MATERIAL AND METHODS
Study populations and Zn supplementation status
The COVID-19 incidences and mortality data (12 March to 26 June 2020) collected from (6). Twenty-three socially similar European populations (Total 522.47 million) with similar confounders (8-12) but different Zn sufficiency/deficiency levels (3), had registered 15.71% cases (1552 thousand cases) and 34.2% deaths (173 thousand deaths) of the total global were analyzed for correlation.
Statistical analysis
All basic statistical analysis including correlation (Pearson’s) and regression analysis were performed in Microsoft Excel. COVID-19 mortality and incidence, without applying extra exclusion/inclusion criterion of risk factor or supposed confounders (e.g., age, sex, age distribution, comorbidities, populations’ density etc.), were assessed for correlation with populations’ Zn sufficiency. Interim case fatality ratio (i-CFR) for the populations/groups were calculated as ‘(reported deaths/reported cases)*100. P-value <0.05 is referred to as statistically significant.
Epidemiological Map display and required color manipulation
Global maps showing country-wise Zn-levels as well as COVID-19 incidence and deaths are adapted from [7]. Color scheme variations in maps were performed using ‘Inkscape’.
Data Availability
All data are available in the manuscript/references provided.
Funding
No specific source of funding was utilized for the current study. However, SS acknowledges the funding support to his laboratory from Institute of Eminence (IoE) seed grant, Banaras Hindu University.
Conflict of interest
There is no conflict of interest to disclose.
Ethical statement
The study is compliant with the ethical standards. Considering the design of the study no human or animal rights were infringed upon.
Informed consent
Considering the design of the study no informed consent was necessary.
ACKNOWLEDGEMENTS/ DISCLOSURES
REFERENCES




