
Abstract
Background & Aims Patient infected with the SARS-COV2 usually report fever and respiratory symptoms. However, multiple gastrointestinal (GI) manifestations such as diarrhea and abdominal pain has been described. The aim of this study was to evaluate the prevalence of GI, liver function test (LFT) abnormalities, and mortality of COVID-19 patients.
Methods We performed a systematic review and meta-analysis of published studies that included cohort of patients infected with SARS-COV2 from December 1st, 2019 to July 1st, 2020. We collected data from the cohort of patients with COVID-19 by conducting a literature search using PubMed, Embase, Scopus, and Cochrane according to the preferred reporting Items for Systematic Reviews and MetaAnalyses (PRISMA) guidelines. We analyzed pooled data on the prevalence of overall and individual gastrointestinal symptoms, LFTs abnormalities and performed subanalyses to investigate the relationship between gastrointestinal symptoms, geographic location, fatality, and ICU admission.
Results The available data of 17,802 positive patients for SARS-COV2 from 120 studies were included in our analysis. The most frequent manifestations were diarrhea (13.3%, 95% CI 12-16), nausea (9.1%, 95% CI 9-13) and elevated LFTs (23.7%, 95% CI 21- 27). The overall and GI fatality were 7.2% (95% CI 6 -10), and 1% (95% CI 1- 4) respectively. Subgroup analysis showed non statistically significant associations between GI symptoms/LFTs abnormalities and ICU admissions (OR=3.41, 95% CI 0.87 – 13.4). The GI mortality rate was 0.58% in China and 3.5% in the United States (95% CI 2 - 5).
Conclusion Digestive symptoms and LFTs abnormalities are common in COVID-19 patients. Our subanalysis shows that the presence of gastrointestinal and liver manifestations does not appear to affect mortality, or ICU admission rate. However, the mortality rate was higher in the United States compared to China.
Introduction
In December 2019 China was struck with a new strain of Coronavirus, Novel Coronavirus (2019 nCov). Within a short period of time, it soon spread to a full pandemic.
It was first noticed by the innumerable cases of pneumonia that suddenly surged amongst local inhabitants in the Province of Wuhan. Soon, the virus was detected through sequencing leading to officially being renamed severe acute respiratory syndrome coronavirus 2 (SARS-COV2) by the International Committee on Taxonomy of Viruses [1-2]. The disease caused by Coronavirus (SARS-COV2) was allocated the title of COVID-19 or ‘Coronavirus disease’ [3]. Coronaviruses in general are single stranded RNA viruses falling under the family of Coronaviridae which also include MERS (MERS Cov) and SARS (SARS Cov)[4]. By the end of May, 5,796, 257 cases of COVID-19 have officially been confirmed worldwide and as of July the number of confirmed cases passed the 12 million mark [5].
It has been established that the transmission of Coronavirus (SARS-COV2) occurs from person to person through upper airway tract (droplet infection) or direct contact [6]. The virus can also be detected in saliva, urine, gastrointestinal tract and possibly through airborne spread [7,8]. The spectrum of symptoms attributable to SARS-COV2 include fever, cough, myalgia, fatigue, and to a lesser extent headache. Patients may also be asymptomatic [9-11]. Diarrhea, nausea and vomiting, as well as liver involvement have all been reported in the literature [12,13]. In fact, gastrointestinal involvement is plausible given that angiotensin converting enzyme 2 (ACE2), the major human cellular receptor for the SARS-COV2, is expressed in the gastrointestinal tract as well as liver cells [14]. We thus conducted a systematic review of published gastrointestinal and liver symptoms associated with COVID-19 on the basis of disease severity, age group, and geographical region.
Methods
Search strategy
A systematic review was conducted using Pubmed, Scopus, Cochrane, and Embase databases. Medical literature searches for human studies were performed from December 1st, 2019 up to July 1st, 2020. The key terms used for the literature search were ((“COVID-19” OR “COVID 2019” OR “severe acute respiratory syndrome coronavirus 2” OR “severe acute respiratory syndrome coronavirus 2” OR “2019 nCoV” OR “SARS-COV2” OR “2019nCoV” OR (“severe acute respiratory syndrome coronavirus 2” OR “SARS-COV2” AND GASTROINTESTINAL AND (MANIFESTATIONS OR CLINICAL CHARACHTERISTICS) OR (“gastrointestinal tract” OR (“gastrointestinal’ AND “tract”) OR “gastrointestinal tract” OR (“gi” AND “tract”) OR (“fatality” or “Mortality”). In addition, a manual search of all review articles, editorials and retrieved original studies was also performed. All procedures used in this meta-analysis were consistent with the Preferred Reporting Items for Systematic Reviews and Meta analyses (PRISMA) guidelines and prespecified protocol, which described our method and analysis before data collection was initiated (see supplementary PRISMA check list).
Selection criteria and data extraction
Data were independently abstracted based on our protocol by two investigators (MS and FA) and any discrepancies between the two authors were resolved through discussion. Inclusion and exclusion criteria were defined prior to the literature search. The inclusion criteria were (1) study type: case reports/case series (including chart reviews), prospective/retrospective cohort studies, case control studies, cross sectional studies and randomized controlled trials; (2) patients population: Adults patients with COVID-19; inpatient or outpatient setting and (3) Outcome measured: At least one GI manifestation reported and LFT abnormality, defined as any value above the normal upper limit.
Exclusion criteria were (1) Review, opinion, abstracts from conferences, editorials, commentary articles, review articles and meta analyses; (2) studies without data for retrieval; (3) duplicate studies; (4) Asymptomatic patients with COVID-19: (5) studies that did not report gastrointestinal symptoms.
Data extraction was performed using Microsoft excel. The following data were extracted:
Study: author, journal, date, country, number of patients, and study type.
Patients characteristics: mean age, ethnicity, gender, and comorbidities.
Overall fatality rate and fatality rate by country.
Number of patients admitted to the ICU.
Gastrointestinal symptoms proportion: abdominal pain, diarrhea, nausea, anorexia, loss of taste, elevated liver enzymes or other nonspecified gastrointestinal symptoms.
Risk of bias and certainty of evidence
The Methodical Index for Nonrandomized Studies (MINORS) [15] was used to assess bias risk (see table 2). In addition, risk of bias was assessed based on 4 domains: selection, ascertainment, causality, and reporting. An overall judgment of risk of bias was made based on factors deemed to be most critical for the systematic review (selection criteria, ascertainment of outcome, and followup duration).
Statistical Analysis
Our primary analysis focused on assessing the weighted pooled prevalence of GI symptoms/LFT abnormalities in patients with COVID-19 infection, occurring any time during the course of illness. We also conducted subanalyses that looked at the association between GI symptoms/LFT abnormalities and mortality as well as ICU admission. Categorical variables were described as count (%). Continuous variables were described using mean (SD) if they are normally distributed, median (IQR) if they are not. We pooled the single arm event rates using a random effects method and we measured heterogeneity within our studies using the I2 statistic. Subanalyses were described and tested using odd ratios and 95% confidence interval to determine statistical significance. Stata 16 was used to calculate odd ratios and their respective 95% CI and create Forest and Box plots.
Sensitivity Analysis
To examine the effect of the quality of studies on our results, we performed a sensitivity analysis on the prevalence of GI symptoms and LFTs abnormalities by excluding low qualities studies. These include case reports, case series and case control studies. We also assessed selected outcomes comparing patients with versus without GI/LFTs abnormalities.
RESULTS
Research selection and quality assessment
Overall, 120 studies (supplementary table. S1) from 2355 potentially relevant citations were included in the analysis (Figure 1). Most of the included studies were single arm only, very few studies included comparator groups. Furthermore, outcome assessors in all 120 studies were not blinded. Both inpatients and outpatients studies were included. The risk of evidence imprecision was rated as very serious, given that the included studies were all observational studies. Overall, all included studies were rated as having very serious risk of bias because they lacked a control group and had a high risk of confounding and selection bias.
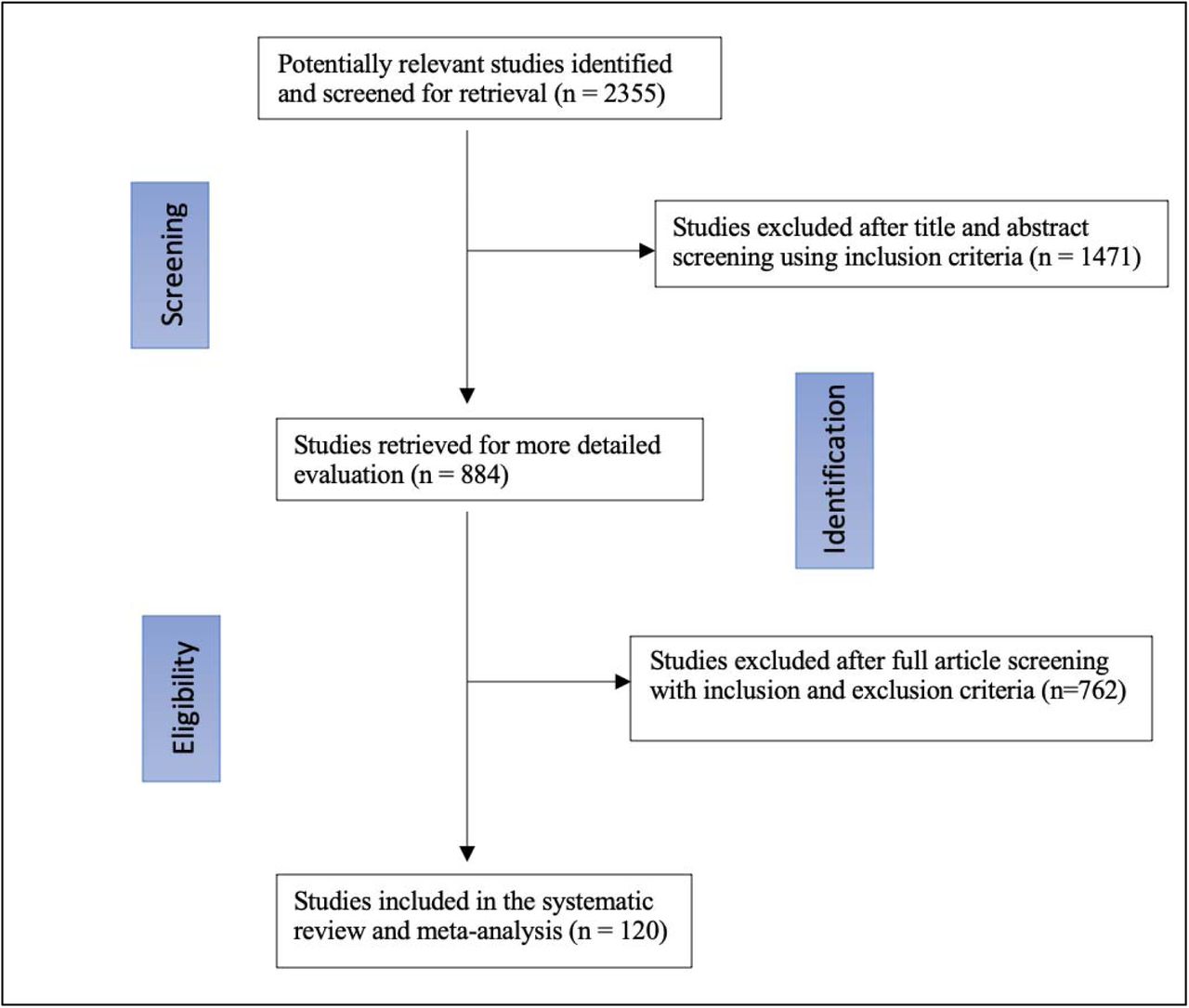
Flow diagram for study selection
Clinical data
This systematic review included 120 studies [16-136] with a total of 17,801 patients that tested positive for SARS-COV2 and were included in the analysis. The mean patient age was 52.6 (±14, 95% CI 48-57.3) and 47.6% of the patients were males. Most patients had several comorbidities, most common being hypertension (23.4%, 95% CI 21-27), diabetes mellites (13.4%, 95% CI, 12-15), and cardiovascular diseases (12.4%. 95% CI, 10-14). GI symptoms included nausea, vomiting, and diarrhea. Heterogeneity statistic I2 is 94.5%, which signifies a significant heterogeneity among our studies. The most common GI/liver manifestations were elevated liver enzymes and diarrhea (supplementary figure.1). Specifically, GI manifestations of patients infected with SARS-COV2 are diarrhea 13.3% (95% CI 12 - 16), nausea (9.1%, 95% CI 9 - 13) anorexia or loss of appetite (8.3%, 95% CI 8 - 11), vomiting (6.4%, 95% CI 5 - 8), abdominal pain (3%, 95% CI, 3-6), loss of taste (1.3%, 95% CI 1 - 4), and elevated LFTs (23.7%, 95% CI 21 - 27).
Sensitivity Analysis
The sensitivity analysis included 25 studies (supplementary: table S4). The results did not differ from our main analysis. Among the GI manifestations experienced by COVID-19 patients, diarrhea (13.1%, 95% CI, 12-14), was still the most common symptom, followed by nausea (9.2%, 95% CI 8-11). The percentage of patients experiencing LFTs abnormalities was 24% (95% CI 21 - 26).
Fatality rates and Geographic Variation
A total of 78 studies reported the incidence of mortality. The overall fatality rate of patients was 7% (95% CI 6 -10), (supplementary: table S5). The subgroup analysis included three studies [19-21] that directly compared mortality rate in patients with and without GI symptoms. In this analysis the number of patients who experienced gastrointestinal symptoms/liver test anomalies and those who did not were 227 and 326, respectively. The results showed that patients with GI manifestations//LFT abnormalities were no more likely to die compared to those who did not with a pooled odd of patients was not statistically significant 1.07 (95% CI 0.58 - 1.97) (figure 3).

Box plots representing the range and outliers of the gastrointestinal and liver manifestations in patients with COVID-19.

Forest Plot for mortality in patients with COVID-19, showing no significant difference in the pooled odds of patients with gastrointestinal symptoms and those without gastrointestinal adverse events.
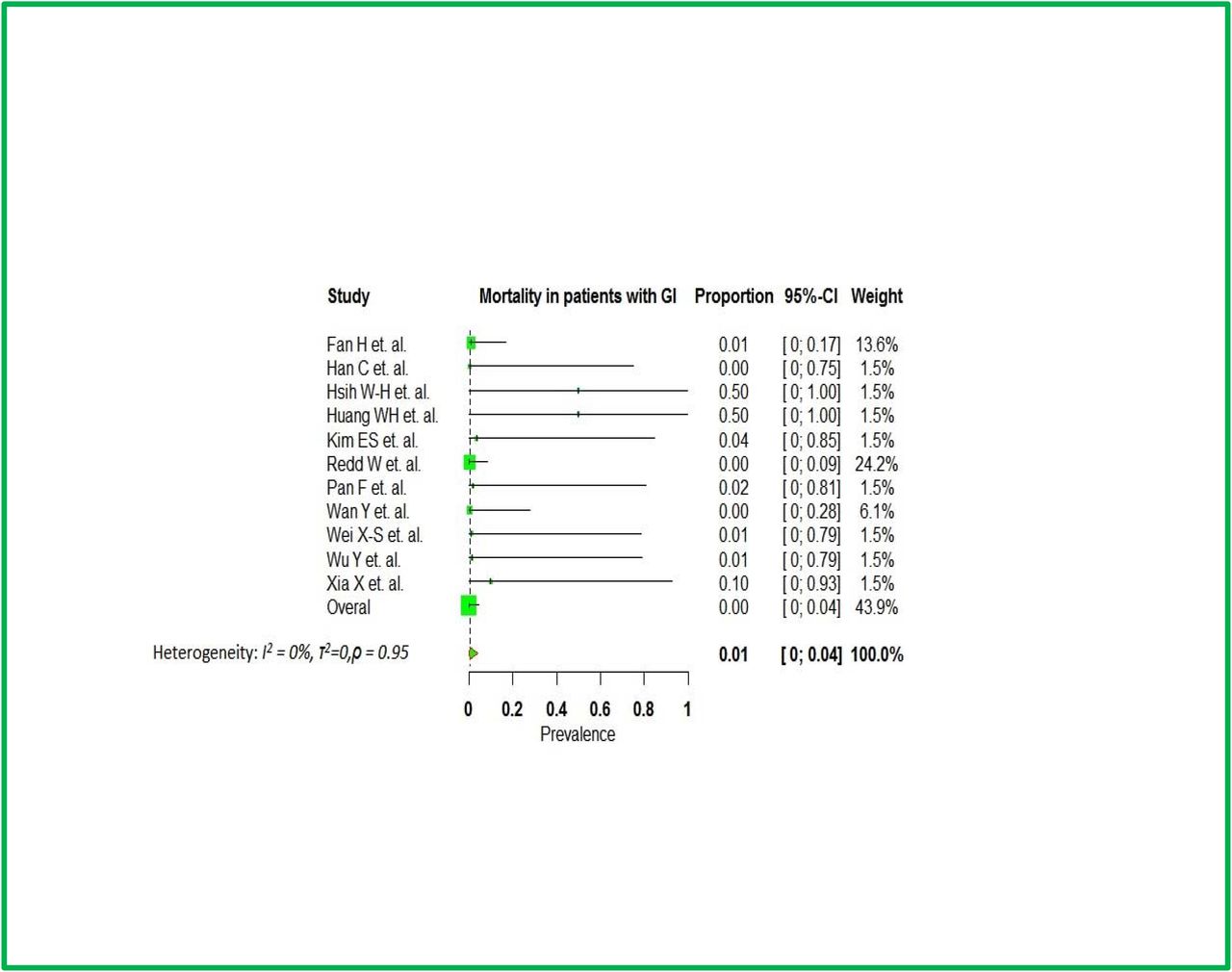
Moreover, out of the 78 studies, a total of 25 studies reported mortality in patients with GI/Liver manifestations (see figure 4). A subanalysis of fatality rate in patients with GI symptoms based on their location showed that 27 out 4660 patients (0.58%) in China died (95% CI 0.5, 1.6), whereas 16 out 449 patients (3.5%) in the United States died (95% CI 2 - 5). In addition, 3 studies from Taiwan, Korea, and Japan reported zero fatality (table.1).
Mortality by geographic location

Funnel plot of the 25 studies that reported mortality of patients with GI symptoms
ICU admission rate
Only two studies [20,21] reported differences in ICU admissions amongst patients manifesting GI symptoms/LFT abnormalities and patients without. The total number of patients with gastrointestinal problems or LFT abnormalities who were admitted in the ICU were 23 and the number of patients who did not experience gastrointestinal problems or LFT abnormalities and were admitted to the ICU were 156. No statistically significant difference in ICU admission rate was noted between those who experienced GI/LFTs abnormalities and those who did not. The pooled proportion was 3.41 (95% CI, 0.87,13.4). (Figure. 5).
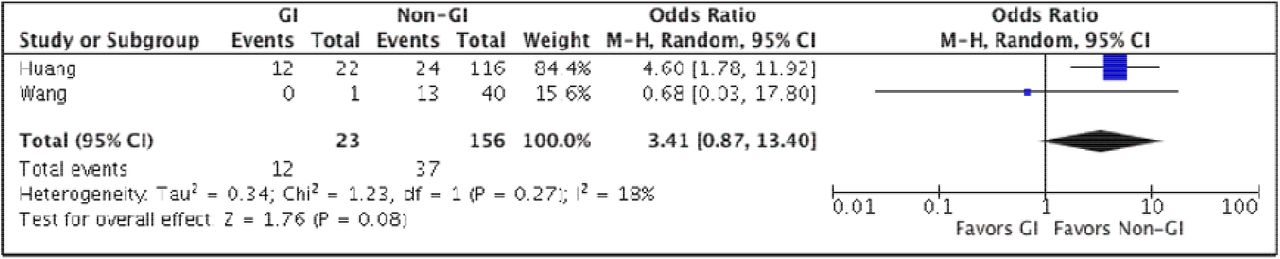
Odds ratio of ICU admissions in patients with COVID-19amongst patients with and without gastrointestinal symptoms / LFT abnormalities.
Discussion
This meta-analysis of 17,801 COVID-19 patients found that gastrointestinal symptoms are common in patients infected with SARS-COV2. Our study has several strengths. This is one of the more recent meta-analyses that summarizes the rapidly emerging and sometimes confusing literature on COVID-19 on the prevalence of overall and individual gastrointestinal manifestations. The large patient population and comprehensive inclusion of 120 studies allow a more precise estimation of the prevalence of gastrointestinal symptoms and liver test anomalies associated with COVID-19. Subgroup analysis found that no association between the presence of gastrointestinal symptoms/LFT anomalies and mortality; but a trend towards their absence and ICU admission was noted.
Gastrointestinal symptoms including abdominal pain, diarrhea, nausea, vomiting, loss of appetite, loss of taste and elevated liver enzyme are among the presenting symptoms or laboratory abnormalities of SARS-COV2 infection. Diarrhea was the most common gastrointestinal symptom; this is particularly important because previous studies have shown that patients with diarrhea on presentation have a higher stool RNA positivity and viral load than those without [137,138]. One study showed that 44 of 153 patients with COVID-19 tested positive for the virus in the stools [139]. Another study by Xiao et al. showed that among 73 hospitalized COVID-19 patients in China, 39 (53.42%) tested positive for SARS-COV2 RNA in stools [140]. In addition, a report of a COVID-19 patient with positive fecal but negative pharyngeal and sputum viral tests has been described [140]. This may imply that fecal oral route is a possible route of SARS-COV2 transmission.
The possibility of fecal oral transmission of SARS-COV2 emphasizes the importance of frequent and proper hand hygiene. This is important in every clinical setting, but especially in low resource areas with poor sanitation. Intuitively, proper handling of the excreta of COVID-19 patients should still be strongly enforced, and sewage from hospitals should also be properly disinfected. The presence of the virus in the digestive tract also raises the concerns of COVID-19 infection in patients with established gastrointestinal conditions as well as potential fecal microbiota transplant donors. Nevertheless, the unknown effect of COVID-19 on patients with preexisting gastrointestinal diseases and its influence on treatment and outcome is a cause for concern [140]. These implications warrant further investigation. The American Gastroenterological Association (AGA) and joint society recommend the use of enhanced personal protective equipment, including the use of N95 (or N99) masks instead of surgical masks, for health care workers performing upper or lower GI procedures regardless of COVID19 status [141].
It is believed that the prevalence of gastrointestinal symptoms is underestimated because the majority of studies only reported gastrointestinal symptoms on the day of admission but not throughout the disease course [142]. Furthermore, many earlier studies did not report on other gastrointestinal symptoms except for diarrhea [141,143]. Based on these findings, clinicians must be aware that digestive symptoms, such as diarrhea, may be a presenting feature of COVID-19 that can arise before respiratory symptoms, and on rare occasions may be the only presenting manifestation of COVID-19.
The analysis also found that elevated liver enzymes are a common laboratory marker of COVID-19 patients. Huang et al. showed that AST elevation was observed in 8 (62%) of 13 patients in the intensive care unit compared with only 7 (25%) of 28 patients who did not require care in an ICU [140]. On the other hand, one study from China showed that COVID-19 patients with underlying chronic hepatitis B infection did not have higher disease severity compared to the overall population [143]. Unfortunately, most studies report liver enzymes as the mean/median value of the entire cohort without cutoff values for a given institution rather than as a proportion of patients with elevated values. One aspect that remains to be determined is the impact of COVID-19 in patients with preexisting chronic liver diseases, such as viral hepatitis, and fatty liver disease.
The pooled analysis showed that the overall fatality rate was 11.2%. While the finding is not statistically significant, any possible true difference in mortality may be worth further investigation among better defined COVID-19 patient subgroups with GI/LFT anomalies because one study showed that prevalence of severe disease was more common in patients who had gastrointestinal symptoms than those who did not [141]. Furthermore, a study by Wang et al found that abdominal pain was more frequent in patients who required ICU care than those who did not [142]. Although our finding was not statistically significant, the subgroup sub analysis showed that patients who did not have gastrointestinal manifestations were more likely to be admitted to the ICU. This possible finding also requires additional data.
Limitations
Most of the studies we base our analyses on are observational, single arm cohorts. The lack of control groups and comparison arms can lead to bias due to confounding. Also, our subanalyses might have been affected by small sample sizes. Additionally, regarding fatality rate among COVID-19 patients, most of the studies did not differentiate between the GI symptoms and LFTs abnormalities when performing head to head comparison.
Conclusion
In this meta-analysis, we summarize the recent reports of digestive symptoms/LFT anomalies among patients infected with SARS-COV2. Gastrointestinal symptoms are commonly observed in patients with COVID-19, therefore, clinicians should be aware that diarrhea and nausea can be the only manifestations of COVID-19 patients. Our sub analysis showed that patients infected with SARS-COV2 and exhibiting digestive symptoms had higher mortality rate in the United States compared to China. We also could not find statistically significant association between ICU admission in patients with GI symptoms compared to those without digestive symptoms or hepatic manifestations due to small sample size; however, further investigation is warranted to better assess this possible association.
Data Availability
all data link availabe
Supplemental Material
Studies included in the meta-analysis
The Methodical Index for Non-randomized Studies (MINORS)
Gastrointestinal symptoms
Sensitivity Analysis
Fatality numbers as reported by each study
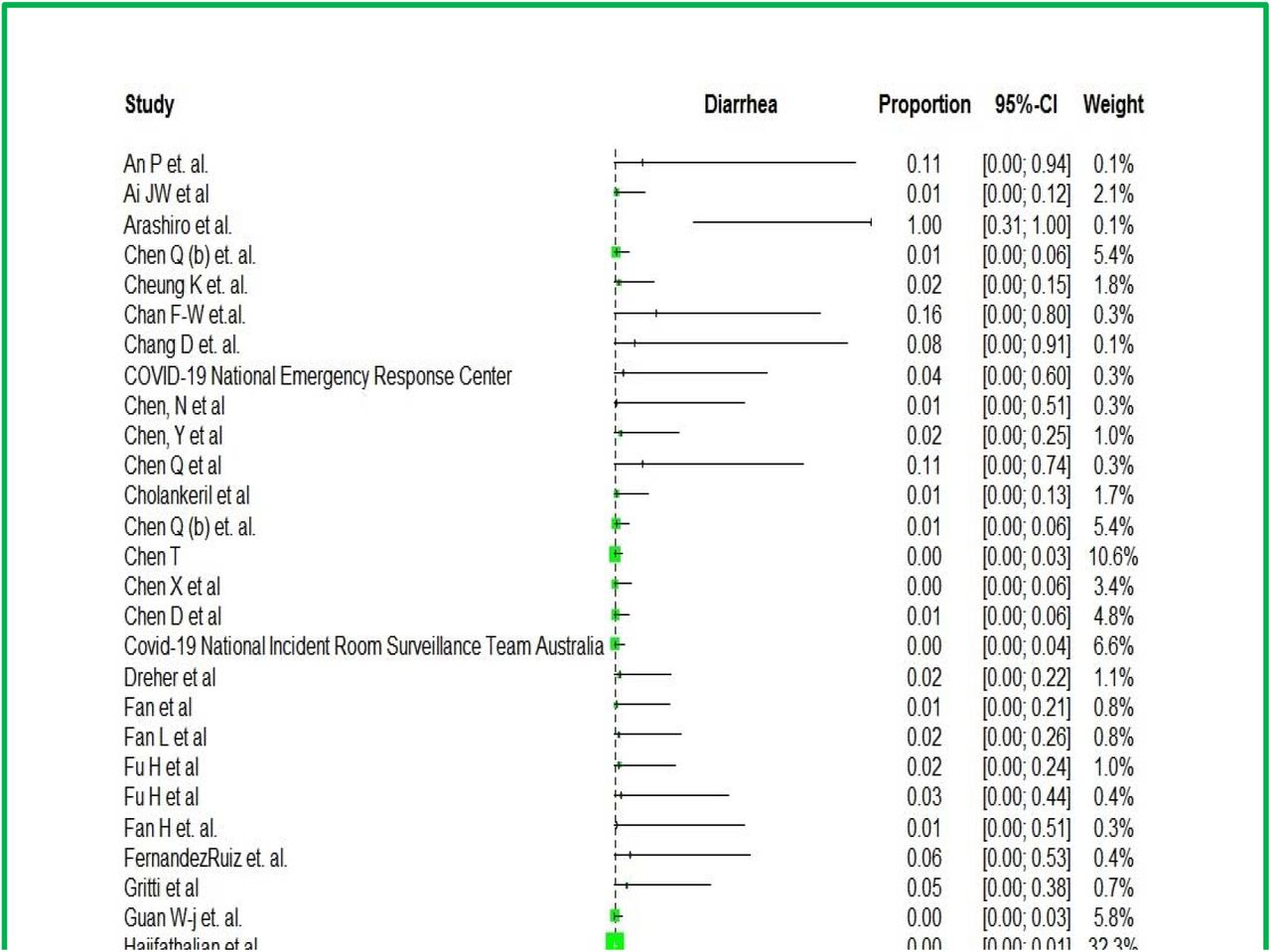
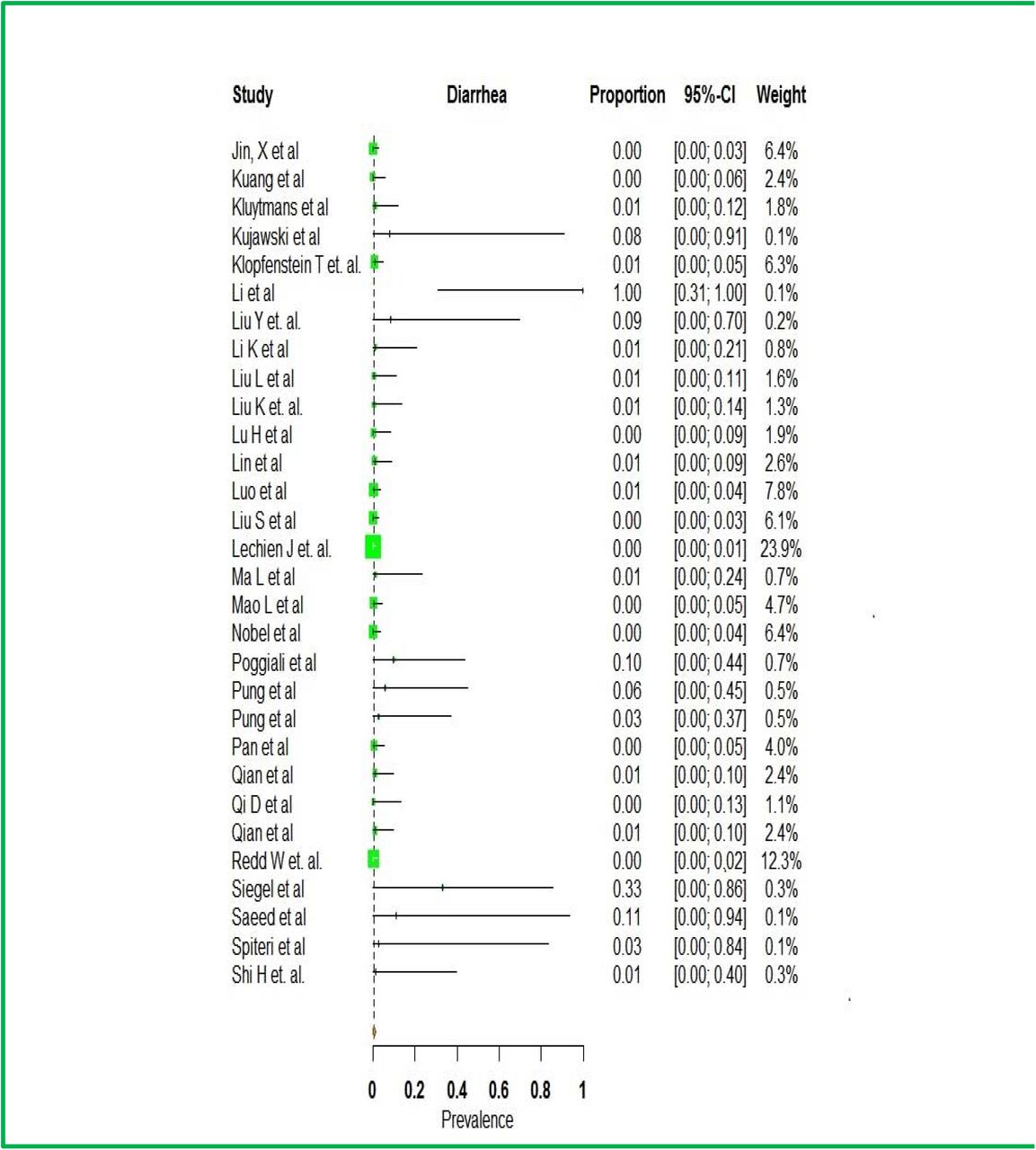

Forest plot depicting prevalence of diarrhea
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Footnotes
Disclosure: All authors have no financial disclosures to report.
References




