
Abstract
BACKGROUND It may take months to years until drugs specifically designed to treat COVID-19 are available. Until then, it is crucial to identify whether existing medications could have a protective effect against severe disease. This is the objective of this large population study performed in Clalit Health Services (CHS), the largest healthcare provider in Israel.
METHODS CHS centrally manages electronic health records (EHRs) including medication purchases for over 4.5 million members. Two case-control matched cohorts were assembled to assess systematically which drugs affected the risk of COVID-19 hospitalization: in both cohorts, case patients were hospitalized for COVID-19; matched control patients were taken from the general population in the first cohort, and non-hospitalized SARS-CoV-2 positive patients in the second cohort. For each medication anatomical-therapeutic-chemical (ATC) class acquired during the last month before the index-date, we computed the odds ratio (OR) for hospitalization, 95% confidence interval (CI), and the p-value, using Fisher’s exact test. False discovery rate was used to adjust for multiple testing.
RESULTS Several drugs and pharmacy sold items were associated with significantly reduced odds for SARS-CoV-2 hospitalization, notably ubiquinone (OR=0.185, 95% CI [0.058,0.458], p<0.001), ezetimibe (OR=0.513, 95% CI [0.375,0.688], P<0.001), rosuvastatin (OR=0.746, 95% CI [0.645,0.858], p<0.001) and flecainide (OR=0.303, 95% CI [0.080,0.813], p<0.01). Additionally, acquisition of surgical masks, latex gloves and several ophthalmological products were associated with decreased risk for hospitalization.
CONCLUSION Ubiquinone, ezetimibe and rosuvastatin, all related to the cholesterol synthesis pathway were associated with reduced hospitalization risk. These findings suggest a promising protective effect which should be further investigated.
Background
SARS-Cov-2 is a new single-stranded RNA virus, which was first identified in December 2019, and has rapidly spread into a global pandemic of primarily respiratory illness designated as Coronavirus Disease 2019 (COVID-19). This disease is associated with significant mortality, particularly among elderly or overweight individuals, raising considerable concerns for public health. Until a vaccine or specifically designed therapies are available, it is urgent to identify whether existing medications have protective effects against COVID-19 complications using available real-world data. With this aim, we performed a case-control study on electronic health records (EHRs) from Clalit Health Services (CHS), the largest healthcare provider in Israel.
Methods
We collected data from the Clalit Health Services (CHS) data warehouse on adult patients aged 18 to 95 years, who had been tested positive for SARS-CoV-2 between the beginning of the pandemics and until September 25, and were admitted for hospitalization through October 10, 2020. Each patient was assigned an index date, which is the first date at which a positive RT-PCR test for SARS-CoV-2 was collected for the patient. Patients’ demographic characteristics were extracted, along with existing comorbidities, clinical characteristics including BMI, and estimated glomerular filtration rate (eGFR) at the baseline, defined as of February 2020. In addition, the list of drugs or products acquired by each patient in CHS pharmacies was collected for the month preceding the index date, defined as 35 to 2 days prior to this date.
Hospitalized COVID-19 patients were assigned to two distinct case-control cohorts, which differ in the way control individuals were selected. In cohort 1, control patients were chosen among the general population of CHS members. Since controls can be selected from among millions of individuals, five controls were selected to match each case (5:1), with comprehensively matched baseline attributes, including age, gender, BMI category, socio-economic and smoking status, chronic kidney disease (CKD) stage for patients with renal impairment, and main comorbidities diagnoses (hypertension, diabetes, chronic kidney disease (CKD), congestive heart failure (CHF), chronic obstructive pulmonary disease (COPD), malignancy, ischemic heart disease). Each control was assigned the same index date as the matched case, provided that the patient was still alive and a member of CHS at this date. EHR data were collected for controls using the same procedure described for cases. This cohort is designed to identify drugs that affect the overall risk for hospitalization for COVID-19, where the effect could combine a decreased risk of detectable infection, and a decreased risk for hospitalization once infected.
In cohort 2, control patients were chosen among patients who had a positive test for SARS-CoV-2 but had not been hospitalized as of October 10, 2020. Given the smaller size of the pool from which controls can be drawn, only two controls were matched for each case patient. Attributes which were matched were the age, gender, smoking status, Adjusted Clinical Groups® (ACG) measure of comorbidity(1) and presence of obesity diagnosis. The index date taken was the date of the first positive SARS-CoV-2 test both for cases and for controls. This cohort is more specifically suited to identify drugs that are associated with a decreased risk for COVID-19 hospitalization in patients who had a proven infection with the virus. In both cohorts, there were a minority of case individuals for which enough matching controls could not be found; these cases were not included in their respective cohorts. Patients who were pregnant since February 2020 were also excluded.
Reliable identification of medications procured for a given month is enabled by the fact that in CHS, distinct prescriptions are issued for each calendar month. When medications are provided in advance for multiple months, the date at which the prescription for each month of treatment begins is recorded.
In each cohort, and for each medication anatomical therapeutic chemical (ATC) class, odds ratio for hospitalization was computed, comparing the number of patients who acquired a medication belonging to the class between 35 days and 2 days preceding the index date, in the case and the control groups. Medications found to be significantly associated with hospitalization were also tested for association with disease severity, using a nested analysis in sub-cohorts of patients from the main cohort grouped by disease severity, according to the scale defined by the World Health Organization (WHO): mild (3), serious (4), severe (5-7), deceased (8).
Based on the results from the two cohorts, which highlighted a significantly decreased risk for ubiquinone, ezetimibe, and a statin, which are often prescribed in combination, we subsequently investigated the association between various combinations of these drugs and the outcomes using the same approach.
This study has been approved by the CHS Institutional Review Board (IRB) with a waiver of informed consent, approval number: COM-0046-20. Patients’ data were extracted and processed from CHS data-warehouse using programs developed inhouse in Python and SQL. Patient data that could identify participants were removed prior to the statistical analyses in accordance to the protocol approved by the CHS IRB.
Statistical analysis
Odds ratios for hospitalization for drugs acquired in the case versus control groups and statistical significance were assessed by Fisher’s exact test. Correction for multiple testing was performed using the Benjamini-Hochberg procedure(2), which gives an estimation of the false discovery rate (FDR) in the list. Statistical analyses were performed in R statistical software version 3.6 (R Foundation for statistical computing).
Results
Through October 10, 2020, 8,681 adult patients between the ages of 18 and 95 had a recorded COVID-19 related hospitalization in the CHS database. The matching procedure was able to identify control individuals from the general population in ratio 5:1 for 6,202 patients in the first cohort, and control patients in ratio 2:1 from 6,919 SARS-CoV-2 positive individuals in the second cohort. The characteristics of the matched populations are shown in Table 1.
Demographics and Clinical characteristics of the two matched cohorts of patients (hospitalized vs. non-hospitalized)
In each of the two cohorts, we counted the number of patients from each group who acquired drugs and other medical products from each Anatomical Therapeutic Chemical (ATC) class and computed the odds ratios and p-values using Fisher’s test. The distribution of odds ratio for drugs for which the p-value was statistically significant (p<0.05) is shown in Figure 1. The odds ratios for most drugs are neutral or associated with an increased risk of COVID-19 hospitalization. Only a small number of items are associated with decreased risk: 1.15% in cohort 1, and 1.75% in cohort 2.

The overwhelming majority of medications are associated with neutral effect (gray) or increased risk for hospitalization (black, OR>1), only a few are associated with significantly decreased risk (black, OR<1)
Table 2 presents the list of drugs and products that were found to be negatively associated with COVID-19 hospitalization in a statistically significant manner in cohort 1 (A) and in cohort 2 (B). We display items for which the p-value is below 0.05, and for which the false discovery rate (FDR) is less than 0.30, meaning that at least 70% of the items in the displayed list are expected to be true positives. Items are sorted in decreasing order of significance.
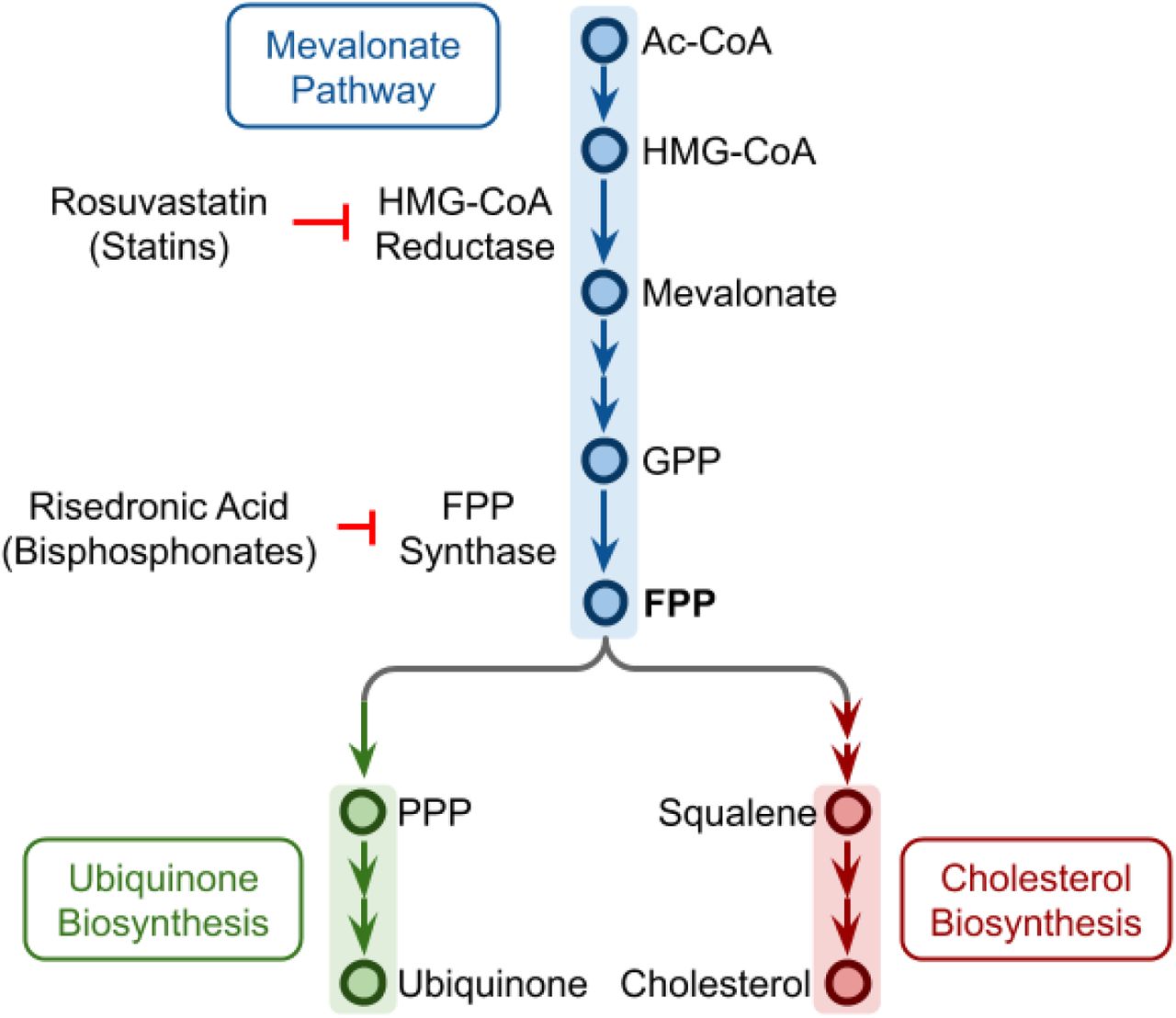
The top ranked medications by significance in both cohorts are ubiquinone, ezetimibe, and rosuvastatin. It is remarkable that these three drugs act on the cholesterol and ubiquinone synthesis pathways, which both stem from the mevalonate pathway(3); the intermediate product at the branch point is farnesyl polyphosphate (FPP) (Figure 2). Rosuvastatin and other statins specifically inhibit he enzyme HMG-CoA reductase. Ubiquinone is a food supplement available over the counter (OTC) in Israel, which is often recommended to patients prone to muscular pain and receiving a statin treatment(4). Since Ezetimibe, statins and ubiquinone are often used in combination, we performed a nested analysis to more specifically evaluate the impact of possible combinations on the risk of hospitalization. Table 3 presents the odds ratio and p-values associated with acquisition of statins, ubiquinone, and ezetimibe alone and in combination in the whole cohort, and in sub-cohorts of hospitalized patients defined by disease severity. Ubiquinone’s protective effect appears to be more pronounced when given in combination with a statin (OR=0.122, P=0.008, first cohort, for hospitalization in moderate condition). To the extent it is possible to assess in our cohorts, the protective effect of ezetimibe appears to be stronger when this molecule is taken without a statin (OR=0.275, P=0.009, second cohort for severe hospitalization), while the effect observed when ezetimibe is taken with a statin seems similar to the effect of the statin alone. Also identified by both cohorts is flecainide, an antiarrhythmic medication, for which the difference in usage rate among hospitalized patients is significant both in cohort 1 and cohort 2. Several additional drugs with a detected protective effect include risedronic acid (OR=0.593 95% CI [0.415, 0.834], p=0.002), a drug usually prescribed for osteoporosis; several drugs acting at synapses and neurotransmitter receptors of different types (escitalopram, bupropion, donepezil, mirabegron); vitamins (vitamin B12 combination, retinol for the eye), and minerals (calcium-zinc, magnesium); finasteride (an anti-androgen, OR=0.000 95% CI [0.000-0.518]) and desogestrel (a progestin); cilazapril (ACE inhibitor); hydrochlorothiazide (diuretic), and sildenafil.
Interestingly, significant protective effect is also observed for several non-drug items that could act as a barrier in both cohorts: surgical masks, latex gloves, eye care wipes (sterile wipes for eye hygiene), artificial tears, and several different eye-drops and ointments.
Most significant associations for medications acquired in the 30 days preceding the index date in two matched cohorts
Examination of the association between combinations of medications associated with the ubiquinone and cholesterol synthesis pathways and the risk of hospitalization, and severity of hospitalization
{kind=link}
{kind=link}
Ubiquinone and cholesterol biosynthesis pathways originate from a branching of the mevalonate pathway at FPP. Rosuvastatin and other statins can inhibit the HMG-CoA reductase, while risedronic acid and other bisphosphonates can inhibit the FPP synthase. Ac-CoA: acetyl coenzyme A, HMG-CoA: hydroxymethylglutaryl coenzyme A, GPP: geranyl pyrophosphate, FPP: farnesyl pyrophosphate, PPP: polyprenyl pyrophosphate.
Discussion
We identified several drugs and products that are significantly associated with reduced odds for COVID-19 hospitalization, both in the general population, and in patients with laboratory proven SARS-CoV-2 infection. Major strengths of our study include: (i) the large sample of hospitalized COVID-19 patients, (ii) the ability to collect comprehensive data about individual demographic and comorbidity characteristics and to build matched case and control populations, (iii) the ability to track hospitalizations and disease severity, owing to a central database established by the Israeli Ministry of Health and, (iv) the capacity to track which drugs and products have been acquired by patients in the period that have preceded SARS-CoV-2 infection, owing to comprehensive digital systems integration in CHS.
The dual cohort design, with control individuals taken from the general population in the first cohort and from individuals positive for SARS-CoV-2 in the second cohort, with each using different matching criteria, mitigates potential bias that could affect each cohort. The two cohorts allow to evaluate the protective effect of drugs that act either by reducing the initial risk of infection, or by reducing the risk of hospitalization in those infected. Analyses are based on items procured between 35 and 2 days before the initial positive test. This window was chosen in accordance to the monthly renewal of prescription policy in place in CHS, with a blackout of 2 days which was intended to exclude acquisitions related to initial symptoms of the disease.
Limitations of this study are related to it being observational in nature. Best efforts were made to use matching so that patients in case and controls are similar regarding most of the known factors for disease severity, and notably, age, obesity, smoking, and baseline comorbidity. We aimed to get a good tradeoff between controlling for confounding factors by rigorous matching and keeping enough patients so that cohorts are representative of the general population. Our analysis is based on medication acquisition in pharmacies and does not ascertain that medications purchased were used. Notably, some of the drugs associated with a protective effect may have been stopped during patient’s hospitalization so that our analysis may have underestimated the full achievable benefits for some of the drugs. Conversely, since drugs tested here were acquired before patients were positive for SARS-CoV-2, the protective effect of some of the drugs may be fully attained only when treatment is started before or early in the infection.
Bearing these potential limitations in mind, our analyses point to several different viral vulnerability points, which can potentially be exploited to effectively reduce disease severity with drugs that are already available. The drugs identified as protective are ubiquinone, which is a food supplement with a very good safety profile that does not even require a prescription in Israel; rosuvastatin and ezetimibe, two drugs prescribed routinely to reduce cholesterol, and that are considered safe. These findings are in line with previous reports that RNA viruses need cholesterol to enter cells, for virion assembly, and to maintain structural stability(5–8), and that prescribing statins may protect against infection with RNA viruses such as members of family Flaviviridae, including Dengue virus, Zika virus, and West Nile virus(9–11). The involvement of the cholesterol/ubiquinone pathway is further confirmed by the fact that risedronic acid, a drug acting on the enzyme farnesyl pyroposhpate synthase(12) (Figure 2) which catalyzes the production of FPP from which the cholesterol and the Ubiquinone synthesis pathways split(3), is identified as protective as well, even though it is prescribed for osteoporosis regardless of the presence of hypercholesterolemia.
Taken together, our findings lend (albeit indirect) support to the possibility that SARS-CoV2 hijacks the cholesterol synthesis pathway, possibly to boost production of the cellular cholesterol it needs as an RNA virus. The fact that ubiquinone protects against severe disease, suggests that SARS-CoV2 may tilt the mevalonate pathway towards cholesterol synthesis and away from ubiquinone synthesis. Such a pathway imbalance would ultimately result in deficiency of ubiquinone that could lead to cell death unless counteracted by ubiquinone supplementation.
Another medication that appears protective is flecainide, an antiarrhythmic drug that blocks sodium channels in the heart, and inhibits ryanodine receptor 2 (RyR2), a major regulator of sarcoplasmic release of stored calcium ions. It may prevent apoptosis by release of calcium from the ER, once the cell mitochondria cease to function. An expert review recommended that patients with arrhythmia who get COVID-19 should continue flecainide treatment if already prescribed(13). In our study, the protective effect observed in both cohorts is even more marked for severe patients, suggesting that this drug, which can be given intravenously(14), could be administered to patients in respiratory distress, if the protective effect is confirmed in clinical trials.
In addition, several drugs acting on synapses (bupropion, escitalopram, donepezil, mirabegron) were associated with decreased risk of hospitalization. This is consistent with SARS-CoV-2 invading neuronal cells(15), as manifest by symptoms of loss of smell and taste, where it may spread throughout the nervous system across synapses. Decreased neurotransmitter internalization may therefore reduce the infectious potential of the virus.
We also observe protective effects for several vitamins (vitamin B12, vitamin A) and minerals (calcium-zinc, Magnesium). The beneficial roles of vitamin B12, and vitamin A, and zinc have already been mentioned in existing studies(16–18). In a previous report, we have shown that vitamin D deficiency is associated with increased risk of COVID-19(19). Magnesium is needed for vitamin D activation(20) and its levels in drinking water in Israel are low, as water is produced in great part through desalination of sea water(21). The decreased hospitalization rate revealed here for patients taking magnesium supplementation may suggest a role for supplementation of this element along with vitamin D.
Finally, items that could act as a barrier were among the top items decreasing odds of hospitalization, including surgical masks, latex gloves, eye wipes, eye drops, and ointments. Interestingly, the protective effect for these items is observed foremost among patients from cohort 2 in which controls are already SARS-CoV-2 positive. This suggests that barrier items could not only protect against the initial risk of infection, but, notably, also reduce disease severity in patients already infected. In our cohorts, we observe a beneficial effect for many different ophthalmologic preparations, which raises the possibility that autoinoculation of the virus to the eyes, prevented by these preparations, has a role in the virulence of SARS-CoV-2. The possibility that invasion of the central nervous system (CNS) by the virus through the eyes could increase the risk of COVID-19 complications is also supported by the fact that eyeglass wearers were shown previously to be at decreased risk for COVID-19 hospitalization(22). Until the meaning of these findings is fully understood, it may be helpful to advise COVID-19 patients to avoid touching their eyes in order to reduce the risk of complications.
In conclusion, considering the observed protective effects of ubiquinone, ezetimibe, rosuvastatin, risedronate and flecainide in this large population analysis, we recommend to further investigate these and other products identified by this study, in prospective trials aimed to reduce disease severity in COVID-19 patients. In the meantime, we believe that the observed protective effects of these drugs provide important evidence supporting their safe continuation in hospitalized COVID-19 patients.
Data Availability
This study is based on patients' clinical data and cannot be shared outside of Clalit Health Services
Contributors
All authors provided final approval to publish. AI, IF and AT had access to the raw data. AI designed the study. AI, AS, AC, IF, AT, KC, SS, ES, ER and GL contributed to data analysis and interpretation. AI, AS, ER and GL contributed to the drafting of the article.
Declaration of interests
The authors declare no conflict of interest
Funding
This research was supported in part by the Intramural Research Program of the National Institutes of Health, NCI.
Footnotes
Manuscript revised, Table 3 corrected, Figure 2 added




