
Abstract
Background Smoking impairs lung immune functions and damages upper airways, increasing risks of contracting and severity of infectious diseases.
Methods We searched PubMed and Embase for studies published from January 1-May 25, 2020. We included studies reporting smoking behavior of COVID-19 patients and progression of disease, including death. We used a random effects meta-analysis and used meta-regression and lowess regressions to examine relationships in the data.
Results We identified 47 peer-reviewed papers with a total of 31,871 COVID-19 patients, 5,759 (18.1%) experienced disease progression and 5,734 (18.0%) with a history of smoking. Among smokers, 29.2% experienced disease progression, compared with 21.1% of non-smokers. The meta-analysis confirmed an association between smoking and COVID-19 progression (OR 1.56, 95% CI 1.32-1.83, p=0.001). Smoking was associated with increased risk of death from COVID-19 (OR 1.19, 95% CI 1.05-1.34, p=0.007). We found no significant difference (p=0.432) between the effects of smoking on COVID-19 disease progression between adjusted and unadjusted analyses, suggesting that smoking is an independent risk factor for COVID-19 disease progression. We also found the risk of having COVID-19 progression among younger adults (p=0.023), with the effect most pronounced among people under about 45 years old.
Conclusions Smoking is an independent risk for having severe progression of COVID-19, including mortality. The effects seem to be higher among young people. Smoking prevention and cessation should remain a priority for the public, physicians, and public health professionals during the COVID-19 pandemic.
BACKGROUND
Coronavirus disease 2019 (COVID-19) first occurred in Wuhan, China in December 2019 and has spread rapidly around the world. As of June 2020, the virus had infected over 6 million people and caused more than 300,000 deaths. Old people and those with pre-existing medical conditions including respiratory disease, hypertension, diabetes, cardiovascular disease, and cancer are more vulnerable to becoming critically ill when infected [1].
Smoking appears to enhance the risk of COVID-19 by its biological effects and behaviors of smokers. Smoking impairs lung function and pulmonary immune function, compromising the body’s defense mechanisms against infections [2]. Smoking is also a well-established risk factor for chronic diseases that are linked to more severe COVID-19. The World Health Organization (WHO) has advised the public that smoking could increase the risk of contracting COVID-19 because the behavior of smokers involves contact of fingers with the lips and removal of the protective face masks to smoke [3].
Our recent meta-analysis of the 19 peer-reviewed papers found that smokers have double the odds of COVID-19 progression risk [4]. Some people argue that the association between underlying health conditions and risk factors such as smoking to the severity of COVID-19 is still unclear due to inadequate adjustment of confounding factors [5]. In addition, it is unclear whether the association between smoking and severity of COVID-19 varies by age. This paper updates and extends our previous meta-analysis [4] of 19 studies to add 28 additional studies, including 7 that provided adjusted odds ratios and compared the association between smoking and COVID-19 disease progression between unadjusted analyses with adjusted analyses to examine whether smoking is an independent risk factor. We also assessed the effect of age of patients and conducted a sub-analysis for the risk of smoking on the mortality of COVID-19.
METHODS
This study followed the Preferred Reporting in Systematic Reviews and Meta-Analyses (PRISMA) guidelines and is registered with PROSPERO (CRD42020186864).
Data source and search strategy
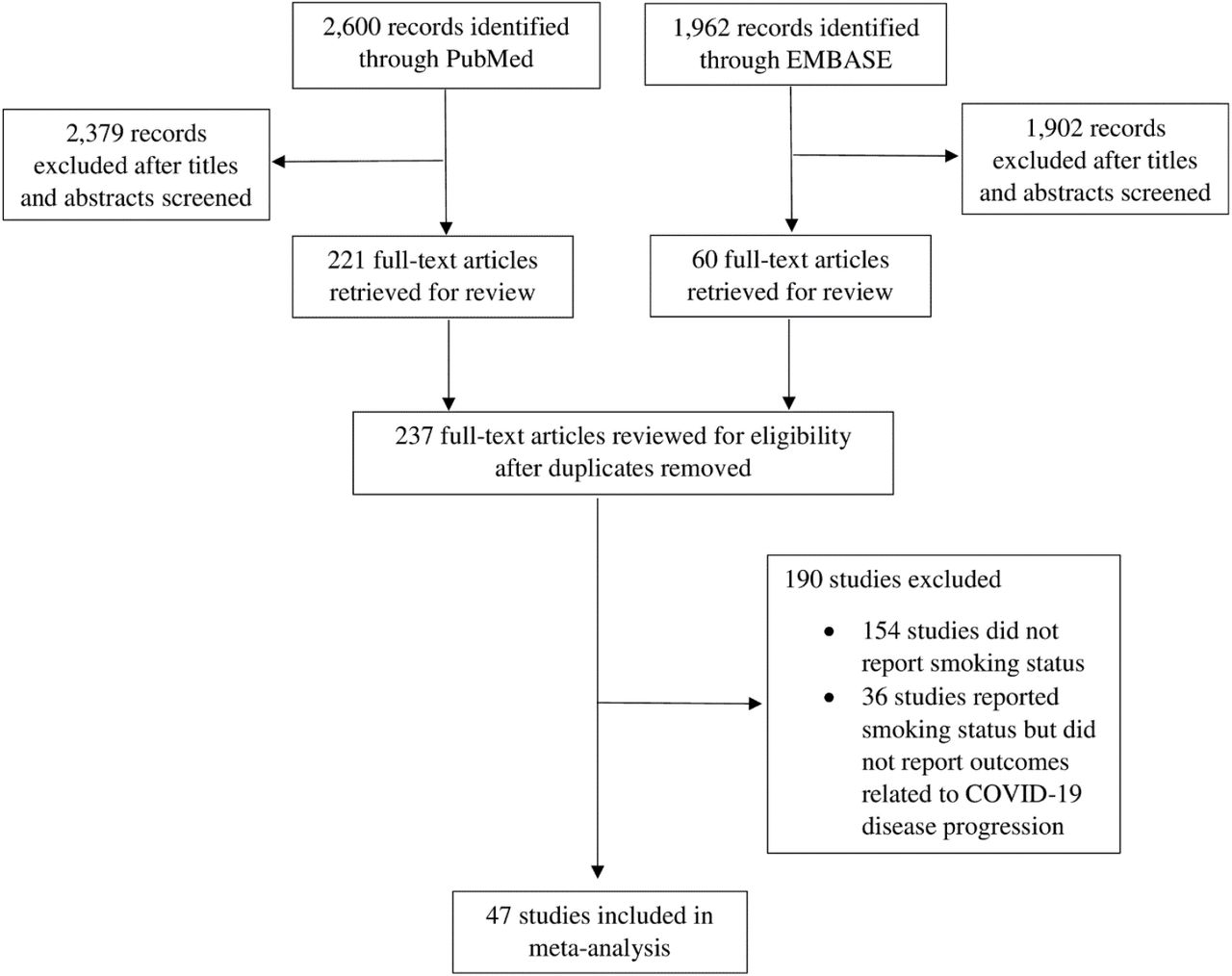
We conducted a systematic search using PubMed and Embase on May 25, 2020, with the search term: “((smoking) OR (characteristics) OR (risk factors) OR (retrospective*) OR (outcomes) OR (smoker*)) AND ((COVID-19) OR (COVID) OR (coronavirus) OR (sars cov-2) OR (sars cov 2))” for studies published between January 1, 2020 and May 25, 2020. A total of 2,600 studies were retrieved through PubMed and 1,962 studies through Embase.
Eligibility criteria
Eligible studies included published peer-reviewed observational studies, retrospective cohort studies, prospective cohort studies, cross-sectional studies, case series, and case reports that reported demographic characteristics, comorbidities specifically smoking status, clinical manifestations, and clinical or disease outcomes of COVID-19 patients on disease progression of COVID-19 to more severe or critical conditions or death. We included both inpatient and outpatient settings. We excluded studies that did not report smoking status and outcomes, studies of children, studies that included other coronavirus infection and not specifically to COVID-19, studies that the number of smokers was zero or omitted, and studies in which all patients had the same outcome. There were no language restrictions.
Study Selection and Data Extraction
One author (RP) extracted information for each study, screened the abstract or the full text, with questions resolved through discussion among both authors (Figure A1).
The exposure group for our analysis were those who had a history of smoking (current smokers or former smokers) and unexposed group was never smokers, non-smoker, or not having a smoking history. Outcomes were progression of COVID-19 to more severe or critical conditions or death. Definitions of smoking status and disease progression for each study are shown in Table A1.
Quality Assessment
We evaluated the quality of studies using a modification of the ACROBAT-NRSI[6] tool on 5 domains: study population, exposure measurement, outcome assessment, measurement of confounders, and adequate follow-up. Each one of these domains was scored from 0 (low risk of bias) to 2 (high risk of bias) and the average score of each study was computed and discussed among both authors (Additional file and Table A2). Studies with the average score higher than 1 were considered high risk and excluded in a sensitivity analysis.
Statistical analyses
Our meta-analyses were based on unadjusted odds ratios (OR) that were either reported in the studies or computed unadjusted OR and 95% confidence interval (CI) using the number of smokers (current and former) and never smokers with and without disease progression. We also did a sensitivity analysis to determine the results changed when the 5 studies with high risk of bias were excluded.
We performed subgroup analyses of (1) the studies that reported association of smoking on COVID-19 mortality and (2) the association of COVID-19 disease progression between current smokers and never smokers (i.e., excluding former smokers) using the studies that reported whether the patient was a current, former, or never smoker (as separate categories).
We also computed the pooled adjusted OR using the studies that reported adjusted OR and 95% CI and compared it with the pooled unadjusted OR.
The results of the included studies were performed with random-effect models using the Stata version 14.0 metan command and metabias command with Egger’s test for the presence of publication bias. We used metareg command (with dummy variables to account for the pairing of adjusted and unadjusted ORs) to determine whether the adjustment of OR affected the results. To examine the effects by age, we used lowess command to generate a nonparametric fit estimate of the relationship between odds of disease progression and mean age of each study. We also tested for a trend using metareg command with mean age of each study as a continuous variable.
RESULTS
Study characteristics
From the total of 4,562 studies we found from our search, 237 studies were considered retrospective cohorts, prospective cohorts, or case series that provided clinical and demographic characteristics of COVID-19 patients. From the 237 studies, 83 studies reported smoking status of the patients, but only 47 studies [7-53] reported smoking status and disease progression of COVID-19 that met our inclusion and exclusion criteria (Figure A1).
Of the 47 studies (Table S1), 33 [10-13, 17-21, 23, 26-29, 31, 35, 37-53] were from China, 8 [8, 9, 14, 16, 22, 25, 33, 34] from the US, 3 [15, 32, 36] from Italy, 1 [7] from the UK, 1 [24] from South Korea, and 1 [30] from 11 countries in Asia, Europe, and North America (China, Japan, South Korea, Turkey, Spain, Italy, Germany, France, UK, Canada, and US).
Eight studies [9, 11, 17, 26, 30, 34, 36, 49] assessed whether the patient was a current, former, or never smoker (as separate categories), 15 [12, 14, 16, 20, 31, 39-43, 45, 46, 50, 51, 53] studies assessed whether the patient was a “current smoker”, 24 [7, 8, 10, 13, 15, 18, 19, 21-25, 27-29, 32, 33, 35, 37, 38, 44, 47, 48, 52] studies assessed whether the patient had a “history of smoking” (current or former).
Clinical outcome was defined as death in 8 studies [11, 15, 25, 30, 32, 33, 44, 53], intensive care unit (ICU) admission or requirement of mechanical ventilation in 6 studies [7, 9, 14, 16, 20, 22], prolonged viral shredding in 2 studies [42, 43], severe or critical (respiratory distress with respiratory rate ≥ 30/min, or oxygen saturation ≤ 93% at rest, or oxygenation index ≤ 300 mmHg, based on the diagnostic and treatment guideline for SARS-CoV-2 issued by Chinese National Health Committee [54] or the American Thoracic Society guidelines [55] for community acquired pneumonia) in 18 studies, the primary composite end point (ICU admission, the use of mechanical ventilation, or death) in 2 studies [17, 46], abnormal chest imaging in 1 study [51], acute cardiac injury in 1 study [18], progression of disease to more severe status (including increasing oxygen supplement, pneumonia exacerbation, transferred to ICU, and sepsis) in 10 studies [12, 19, 23, 24, 29, 31, 33, 36, 37, 47].
There were 5 studies [7, 12, 14, 32, 38] with high risk of bias scores (Table S2).
Smoking and COVID-19 disease progression
A total of 31,871 COVID-19 patients are included in our meta-analysis, 5,759 of whom (18.1%) experienced disease progression and 5,734 (18.0%) with a history of smoking. Among smokers, 29.2% experienced disease progression, compared with 21.1% of non-smokers. The meta-analysis showed an association between smoking and COVID-19 progression (OR 1.56, 95% CI 1.32-1.83, p=0.001) (Figure 1). There was statistically significant moderate heterogeneity among the studies (I2=45.3%, p=0.001) and no evidence of publication bias (p=0.243).

Smoking and COVID-19 disease progression.
Smoking prevalence was significantly higher among patients with disease progression than those without disease progression (p=0.04 by paired t-test).
Smoking and COVID-19 mortality
Eight studies [11, 15, 25, 30, 32, 33, 44, 53] (n = 13,272) reported death as the outcome of COVID-19 patients. The meta-analysis showed an association between smoking and COVID-19 mortality (OR 1.19, 95% CI 1.05-1.34, p=0.007; Figure S3). There was no evidence of heterogeneity among the studies (I2=0%, p=0.654) and no evidence of publication bias (p=0.632).
Studies of current smokers vs. never smokers
The 8 studies [9, 11, 17, 26, 30, 34, 36, 49] that reported current smokers vs. never smokers yielded an elevated point estimate for the effect of smoking on COVID-19 progression (OR 1.42, 95% CI 0.96-2.1, p=0.079; Figure A4), but it did not reach conventional statistical significance. There was statistically significant moderate heterogeneity (I2=58.6%, p=0.018) and no evidence of publication bias (p=0.390).
Unadjusted vs. Adjusted analyses
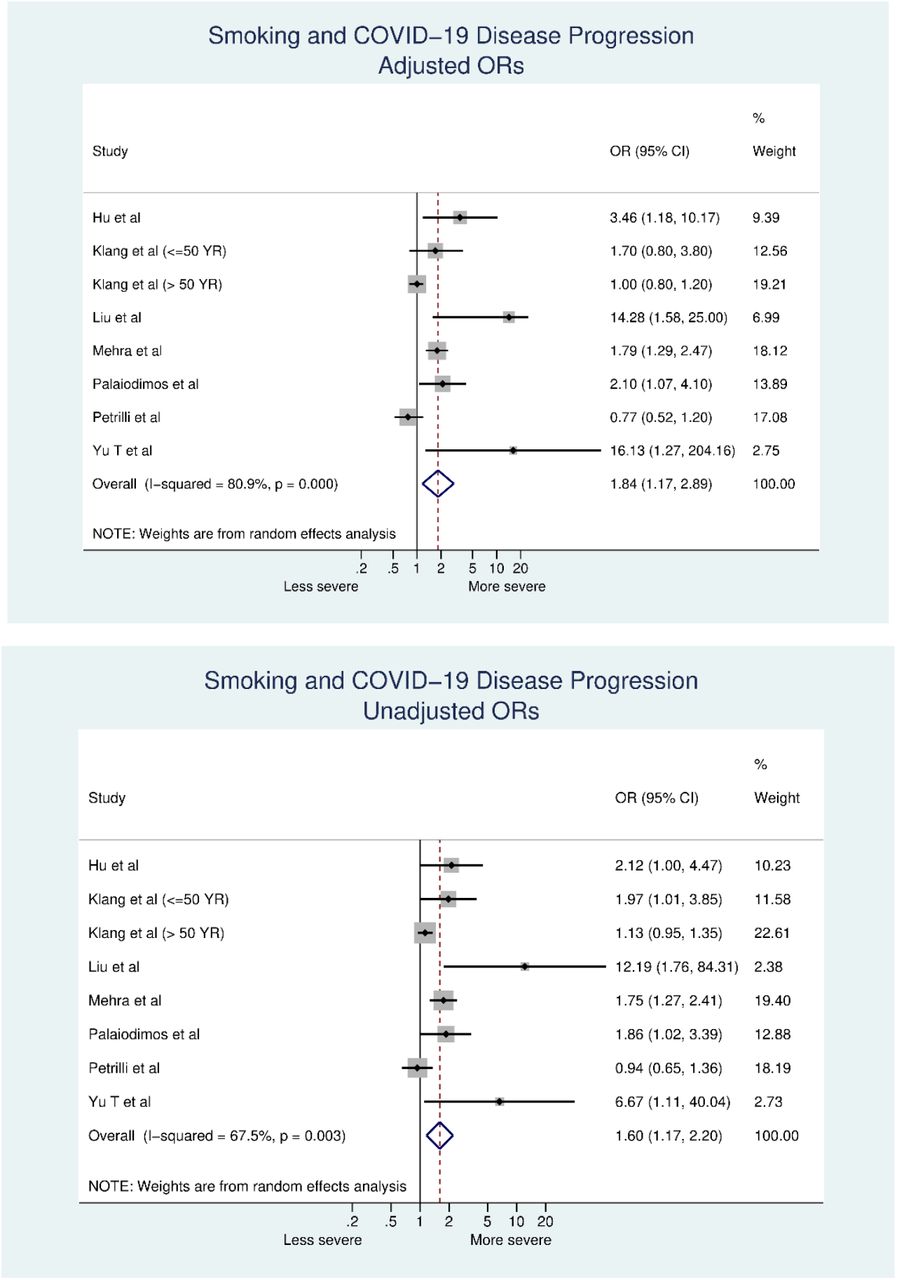
Seven studies [19, 25, 29, 30, 33, 34, 47] reported adjusted ORs. The point estimate for the adjusted ORs (OR 1.84, 95% CI 1.17-2.90, p=0.008; Figure A5, top) was higher than the point estimate for unadjusted ORs (OR 1.60, 95% CI 1.17-2.20, p=0.003; Figure A5, bottom), but this difference was not significant (p=0.432). For the adjusted ORs, the heterogeneity among the studies was high and statistically significant (I2=80.9%, p=0.001) with an evidence of publication bias (p=0.031). For the unadjusted ORs, the heterogeneity among the studies was moderate and statistically significant (I2=67.5%, p=0.003) with an evidence of publication bias (p=0.016).
Association between smoking and COVID-19 disease progression by age
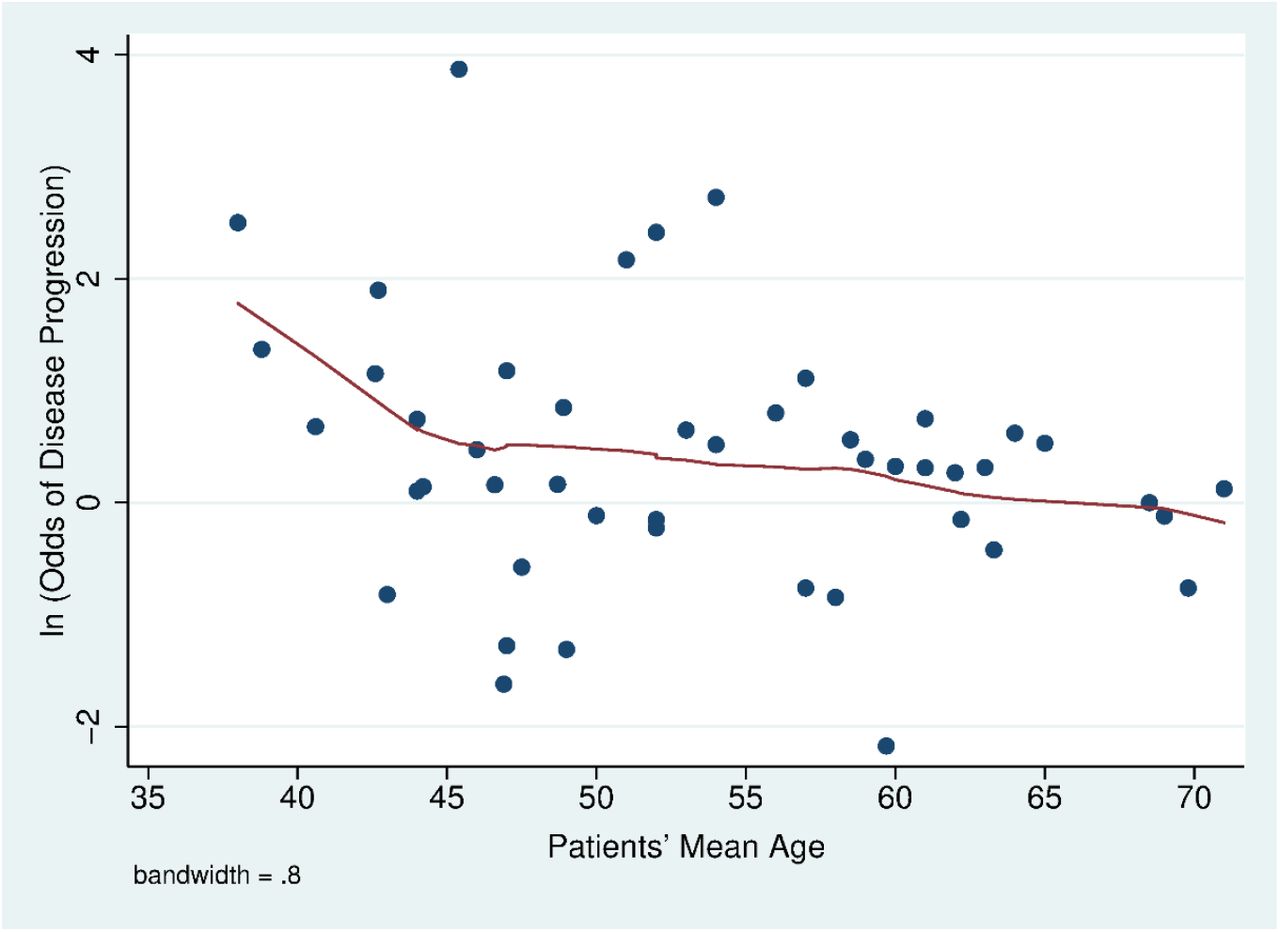
The odds of COVID-19 disease progression between smokers and non-smokers dropped as the patients’ mean age increased across studies, with the drop most pronounced for studies where the mean age was less than about 45 years old (Figure 2). A meta-regression of the odds of COVID-19 disease progression between smokers and non-smokers and the patients’ mean age showed that each the odds of disease progression dropped statistically significantly by a factor of 0.82 (95% CI 0.69-0.97, p =0.023) per 10 years.

As the mean age of patients in a study falls the odds of COVID-19 progression increases. Solid line fit using a lowess regession.
Sensitivity analysis
Dropping the 5 studies [7, 12, 14, 32, 38] with high risk of bias scores had little effect on the odds of COVID-19 disease progression (OR 1.57, 95% CI 1.32-1.86, p=0.001; Figure S2). The heterogeneity among the studies was moderate and statistically significant (I2=50.6%, p=0.001) and there was no evidence of publication bias (p=0.169).
DISCUSSION
With more than twice as many studies available compared to our earlier meta-analysis [4], smoking remains a risk factor for COVID-19 disease progression, with smokers having 1.56 times the odds of progression in COVID-19 severity than non-smokers (Figure 1). The risk of smoking on COVID-19 disease progression was not changed significantly by adjusting for confounders, which suggests that smoking is an independent risk of COVID-19 progression. We also find that smokers are at increased risk of death from COVID-19 (Figure A3). These findings are not surprising because the well-established evidence that smoking is associated with a higher risk of viral infection [2]. In the past pandemics such as influenza [2] and Cov-MERS [56] smoking is also among leading risk factors for worse outcomes.
Young smokers appear to have a higher risk of COVID-19 disease progression than older smokers (Figure 2). A recent study also found that young adults are more medically vulnerable to severe COVID-19 illness if they are smokers [57]. The greater effect of smoking among young people is particularly important because in the U.S., almost 40% of COVID-19 patients are aged 18-44 years [58], and in China, 44% of COVID-19 patients are adults aged 20-49 years [59]. Even so, younger adults tend to perceiving lesser infection-fatality risks of COVID-19 [60] so that they are less likely to protect themselves from the infection. Our finding is consistent with a recent meta-analysis study [61] which concluded that age was negatively significantly associated with the effect of smoking on COVID-19 disease severity.
While there is not yet direct peer reviewed evidence of the effect of e-cigarette use on COVID-19 risk, the fact that e-cigarettes have similar adverse effects on pulmonary immune function [62] combined with the fact that e-cigarette use is concentrated among younger people, raises concerns and points to the need to collect data on e-cigarette use and COVID-19 risk.
Some have argued that smoking has a protective effect against COVID-19 because of the low prevalence of reported among COVID patients [63-65]. This is not new. There was also rumors that smoking protected patients from developing Cov-SARS during the 2003 pandemic [66]. However, a case-control study of 447 patients showed that smoking did not protect patients from contracting Cov-SARS after adjusting for confounding by age, gender, contact history, and occupation [66].
Reported smoking prevalence in the 33 studies in China ranged from 1.4% to 29.8% (median = 7.3%), which was substantially lower than 27.7% (52.1% for men and 2.7% for women) smoking prevalence in 2015 [67]. Four studies [9, 14, 16, 34] in the U.S. that reported the smoking prevalence among current smokers ranged from 1.3% to 33.3% (median=5.2%), which was also lower than 13.7% (15.6% for men and 12.0% for women) smoking prevalence in 2018 [68]. The other 4 studies [8, 22, 25, 33] in the U.S. reported the ever-smoking prevalence ranged from 13.3%-33.5%, which was also lower than 41.9% (47.2% for men and 37.3% for women) in 2017 [69]. One study [36] in Italy reported the smoking prevalence among current smokers of 3.2%, which was also substantial lower than 21.1% (26% for men and 17.2% for women) in 2016 [70]. The remaining studies that reported the ever-smoking prevalence (2 studies[15, 32] in Italy, 1 study [7] in UK and 1 study [24] in South Korea) were also lower than the countries’ rates (Italy: 16.7%-30% vs.43.9% (50% for men and 38.3% for women) in 2010 [71]; UK: 16.7% vs. 40.2 (44.3% for men and 36.5% for women) in 2018 [72]; South Korea: 18.5% vs.39.1% (81.6% for men and 6.9% for women) in 2015 [73]). These low levels of reported smoking among COVID-19 patients may reflect the difficulty of obtaining accurate smoking histories among seriously ill patients, especially when most medical facilities are operating at or above normal capacity. Despite the fact that the reported levels of smoking have been below population prevalences; however, the reported smoking prevalence among people with worse outcomes was significantly higher than those with less severe outcomes (13.5% vs. 9.7%, p=0.042).
Limitations
The studies used a variety of clinical definitions of disease progression and smoking status (Table A1). The varying definitions of disease progression include severity of disease based on clinical manifestations, development to more severe conditions, increasing oxygen supplements, prolonged viral shredding, organ injuries, ICU admission, and death. These varying definitions likely introduced increased variance in the results.
Moreover, smoking was significantly associated with death – a clearly defined endpoint – in the 8 studies [11, 15, 25, 30, 32, 33, 44, 53] that used this endpoint.
Most studies reported smoking status as having a smoking history which was unclear how they categorized former smokers. Of the 47 studies we reviewed, only 8 [9, 11, 17, 26, 30, 34, 36, 49] reported all three smoking categories (current, former, and never smokers). A meta-analysis of these studies found that current smoking was associated with a similar increase in the point estimate for the odds of disease progression (OR 1.42, 95% CI 0.96-2.1; Figure A4) as the other studies (OR 1.49, 95% CI 1.21-1.84), but the odds for current smoking did not reach conventional statistical significance (p=0.079).
Studies that only describe patient smoking history as “smoking history” or “history of smoking” do not provide enough information to analyze smoking as a risk factor given the fact that time since quitting could have significant influence on the patient’s outcomes.
All these limitations add to misclassification errors, which tend to bias results toward the null, suggest that this analysis underestimates the risk of smoking in terms of increasing COVID-19 severity.
The effects of smoking on COVID-19 disease progression by age reported in our paper is limited to the mean age of the studies. Individual level data on smoking, age, e-cigarette use, demographics and other risk factors are needed to perform a more sophisticated analysis. In addition, most of the studies were retrospective cohorts or case series, there might be recall bias, and could not conclude a causal relationship. Most of the meta-analyses in this study had moderate and statistically significant heterogeneity; the reliability of the meta-analysis might be compromised.
Conclusions
Smoking is an independent risk associated with severe progression of COVID-19, including mortality. The effects seem to be prominent among younger adults. Smoking prevention and cessation should remain a priority for the public, physicians, and public health professionals during the COVID-19 pandemic.
Data Availability
All data used to prepare this paper are available from the cited sources.
Authors’ contributions
RP developed the idea for the study, collected, analyzed the data, and wrote the first draft of the manuscript. SAG assisted with revising and refining the manuscript.
Funding
This work was supported by National Institute of Drug Abuse grant R01DA043950, cooperative agreement U54HL147127 from the National Heart, Lung, and Blood Institute and the Food and Drug Administration Center for Tobacco Products and the Faculty of Medicine Ramathibodi Hospital, Mahidol University, Thailand. The content is solely the responsibility of the authors and does not necessarily represent the official views of NIH or the Food and Drug Administration. The funding sources for this study had no role in the study design, data collection, data analysis, data interpretation, or the writing of the manuscript.
Availability of data and materials
All data used to prepare this paper are available from the cited sources.
Ethics approval and consent to participate
Not applicable
Consent for publication
Not applicable
Competing interests
The authors declare that there are no competing interests.
ADDITIONAL FILE
Risk of Bias Assessment
We evaluated the quality of studies using a modification of the ACROBAT-NRSI[6] tool on 5 domains: study population, exposure measurement, outcome assessment, measurement of confounders, and adequate follow-up. Each one of these domains was scored 0 for low risk of bias, 1 for moderate risk of bias, and 2 for high risk of bias and the average score of each study was computed and discussed among both authors. Studies with the average score higher than 1 were considered high risk and excluded in a sensitivity analysis.
Study population
Low risk: studies included at least 50 patients
Moderate risk: studies included at least 20 patients
High risk: studies included less than 20 patients
Exposure measurement
Low risk: studies reported 3 categories of smoking status: current, former, and never smokers
Moderate risk: studies reported 2 categories of smoking status
High risk: studies reported only 1 category of smoking status
Outcome assessment
Low risk: studies reported a clear definition of outcomes
High risk: studies did not report specific outcomes
Measurement of confounders
Low risk: adjustment for confounders
High risk: unadjusted analyses
Adequate follow-up
Low risk: identify duration of data collection
High risk: duration of data collection is unclear
References
References are the same as cited in the main text.
Summary of Studies
(2=high risk, 1=intermediate risk, 0=low risk)

PRISMA diagram
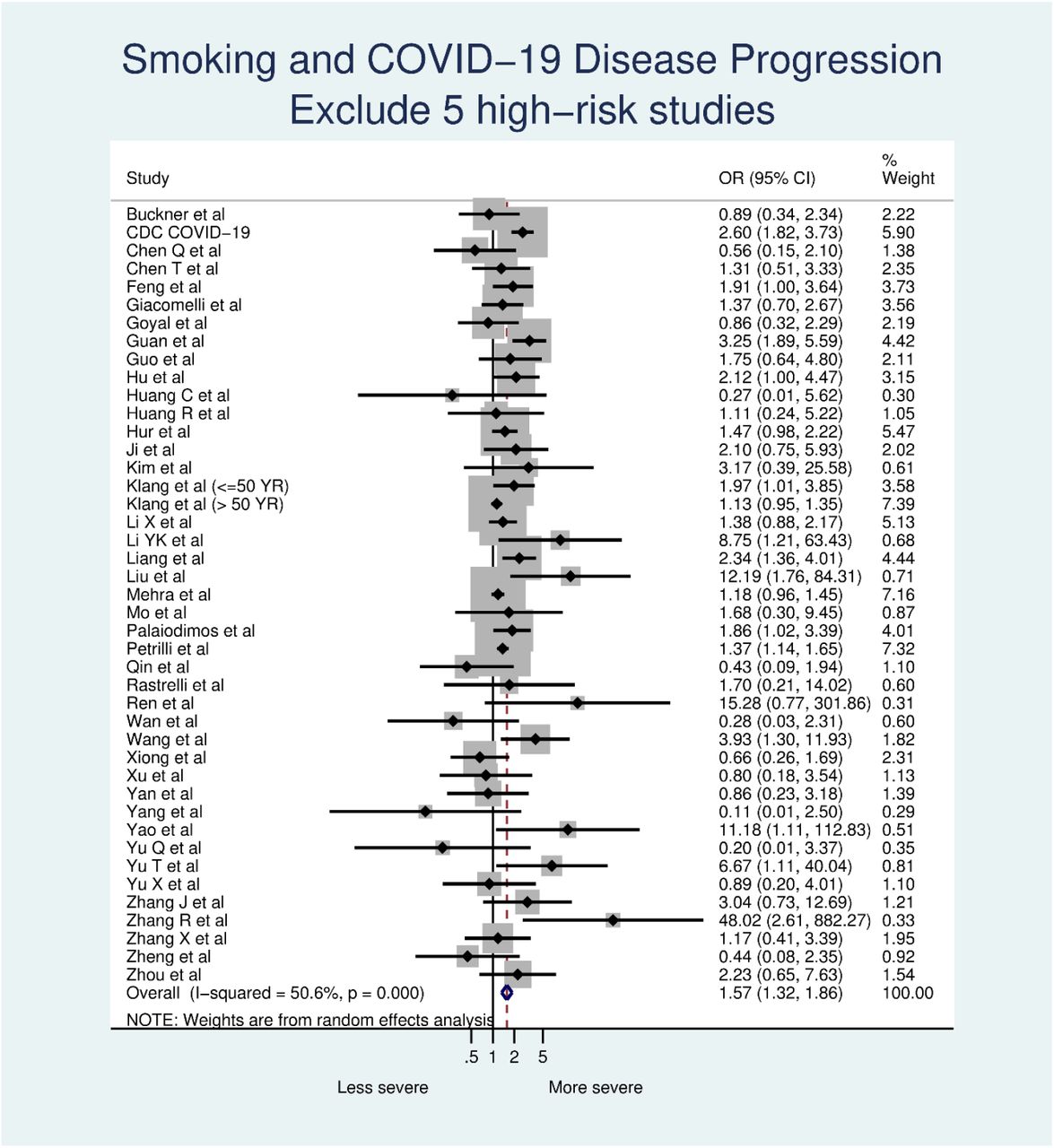
Smoking and COVID-19 disease progression, dropping 5 studies with high risk of bias scores.

Smoking and COVID-19 mortality

Current smokers vs. never smokers and COVID-19 disease progression.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Smoking and disease progression in models that adjusted (top) and did not adjust (bottom) ORs for confounding variables.
Acknowledgement
Not applicable
Abbreviations
- COVID-19
- Coronavirus disease 2019
- CI
- Confidence Interval
- OR
- Odds ratios
- ICU
- Intensive care unit
REFRENCES




