
Abstract
Background Evidence recommends that vitamin D might be a crucial supportive agent for the immune system, mainly in cytokine response regulation against COVID-19. Hence, we carried out a systematic review and meta-analysis in order to maximize the use of everything that exists about the role of vitamin D in the COVID-19.
Methods A systematic search was performed in PubMed, Scopus, Embase, Cochrane Library, Web of Science, and Google Scholar (intitle) as well as preprint database of medRxiv, bioRxiv, Research Square, preprints.org, and search engine of ScienceDirect up to October 10, 2020. Studies focused on the role of vitamin D in confirmed COVID-19 patients were entered into the systematic review.
Results Sixteen studies containing 4922 participants entered into the meta-analysis. The meta-analysis indicated that 48% of COVID-19 patients were suffering from vitamin D deficiency (95% CI, 29%-67%), and in 41% of patients, levels of vitamin D were insufficient (95% CI, 10%-82%). The serum 25-hydroxyvitamin D concentration was 18 ng/mL among all COVID-19 patients (95% CI, 13-24). Co-morbidities frequency in COVID-19 patients were as follows: 7.4% cancer, 27.1% chronic kidney disease, 30.4% cardiovascular diseases, 5.1% dementia, 14.5% depression/anxiety, 32.1% diabetes, 47.4% hypertension, 22.0% obesity and 17.5% respiratory diseases. Reported ethnic groups in studies were 1.0% Afro-Caribbean, 10.3% Asian, and 92.1% Caucasian.
Conclusion This study found that the mean serum 25-hydroxyvitamin D level was low in all COVID-19 patients, and most of them were suffering from vitamin D deficiency/insufficiency. The Caucasian was the dominant ethnic group, and the most frequent co-morbidities in COVID-19 patients were hypertension, cardiovascular diseases, chronic kidney disease, diabetes, obesity, and respiratory diseases, which might be affected by vitamin D deficiency directly or indirectly.
Introduction
Following the emergence of a novel coronavirus from Wuhan, China, in December 2019, the respiratory syndrome coronavirus 2 (SARS-CoV-2) has affected the whole world and is declared a pandemic by World Health Organization (WHO) on March 26, 2020(1). According to Worldometer metrics, this novel virus has been responsible for approximately 37,754,464 infections, of which 28,361,239 cases are recovered, and 1,081,500 patients have died worldwide up to October 12, 2020.
After months of medical communities’ efforts, there is still no specific prevention and treatment approach against the Coronavirus Disease 2019 (COVID-19). Also, a competition of pandemic with infodemic has led to many controversies and challenges globally. In this regard, one of the hottest topics these days is the role of Vitamin D in the prevention or treatment of COVID-19. Several functions, such as modulating the adaptive immune system and cell-mediated immunity, as well as an increase of antioxidative-related genes expression, have been proven for Vitamin D as an adjuvant in the prevention and treatment of acute respiratory infections (2, 3). According to available investigations, it seems that such functions lead to cytokine storm suppression and avoid Acute Respiratory Distress Syndrome (ARDS), which has been studied on other pandemics and infectious diseases in recent years (4-6).
To the best of our knowledge, unfortunately, after several months, there is no adequate high-quality data on different treatment regimens, which raises questions about gaps in scientific works. On this occasion, when there is an essential need for controlled randomized trials, it is surprising to see only observational studies without a control group or non-randomized controlled studies with retrospective nature covering a small number of patients. The same issue is debatable for 25-hydroxyvitamin D (25(OH)D); hence, concerning all of the limitations and analyze difficulties, we carried out a rapid systematic review and meta-analysis to try for maximizing the use of everything that exists about the role of this vitamin in the COVID-19.
Methods
Search Strategy
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guideline was considered for the study plan. A systematic search through databases of PubMed, Scopus, Embase, Cochrane Library, Web of Science, and Google Scholar (intitle), as well as preprint database of medRxiv, bioRxiv, Research Square, preprints.org, and search engine of ScienceDirect, was done up to October 10, 2020. Moreover, to obtain more data, we considered gray literature and references of eligible papers. The search strategy included all MeSH terms and free keywords found for COVID-19, SARS-CoV-2, and Vitamin D. There was no time/location/ language limitation in this search.
Criteria study selection
Four researchers have screened and selected the papers independently, and the supervisor solved the disagreements. Studies met the following criteria included in the meta-analysis: 1) comparative or non-comparative studies with retrospective or prospective nature; and 2) studies reported the role of vitamin D in confirmed COVID-19 patients. Studies were excluded if they were: 1) in vitro studies, experimental studies, reviews, 2) duplicate publications.
Data extraction & quality assessment
Two researchers (H.J and M.M) have evaluated the papers’ quality assessment and extracted data from selected papers. The supervisor (D.Sh) resolved any disagreements in this step. The data extraction checklist included the name of the first author, publication year, region of study, number of patients, co-morbidity, vitamin D Status, serum 25-hydroxyvitamin D levels, ethnicity, mean age, medication dosage, treatment duration, adverse effects, radiological results, and mortality. The modified Newcastle-Ottawa Scale (NOS) checklist for cross-sectional studies was used to value the studies concerning various aspects of the methodology and study process.
Hypothetical strategy
In this case, according to most of the studies, vitamin D cut-off points were considered as follows:
Vitamin D sufficiency: 25(OH)D concentration greater than 30 ng/mL
Vitamin D insufficiency: 25(OH)D concentration of 20 to 30 ng/mL
Vitamin D deficiency: 25(OH)D level less than 20 ng/mL
Targeted outcomes
1) Frequency of Vitamin D status in COVID-19 patients; 2) Mean 25(OH)D concentration; 3) Association between Vitamin D deficiency and COVID-19; 4) Co-morbidity frequency; 5) Ethnicity frequency.
Heterogeneity assessment
I-square (I2) statistic was used for heterogeneity evaluation. Following Cochrane Handbook for Systematic Reviews of Interventions (7), the I2 was interpreted as follows: “0% to 40%: might not be important; 30% to 60%: may represent moderate heterogeneity; 50% to 90%: may represent substantial heterogeneity; 75% to 100%: considerable heterogeneity. The importance of the observed value of I2 depends on (i) magnitude and direction of effects and (ii) strength of evidence for heterogeneity (e.g., P-value from the chi-squared test, or a confidence interval for I2).” Thus, the random-effects model was used for pooling the outcomes in case of heterogeneity; otherwise, the inverse variance fixed-effect model was used. Forest plots were presented to visualize the degree of variation between studies.
Data analysis
Meta-analysis was performed using Comprehensive Meta-Analysis (CMA) v. 2.2.064 software. The pooling of effect sizes was done with 95% Confident Interval (CI). The fixed/random-effects model was used according to heterogeneities. In the case of zero frequency, the correction value of 0.1 was used.
Publication bias & sensitivity analysis
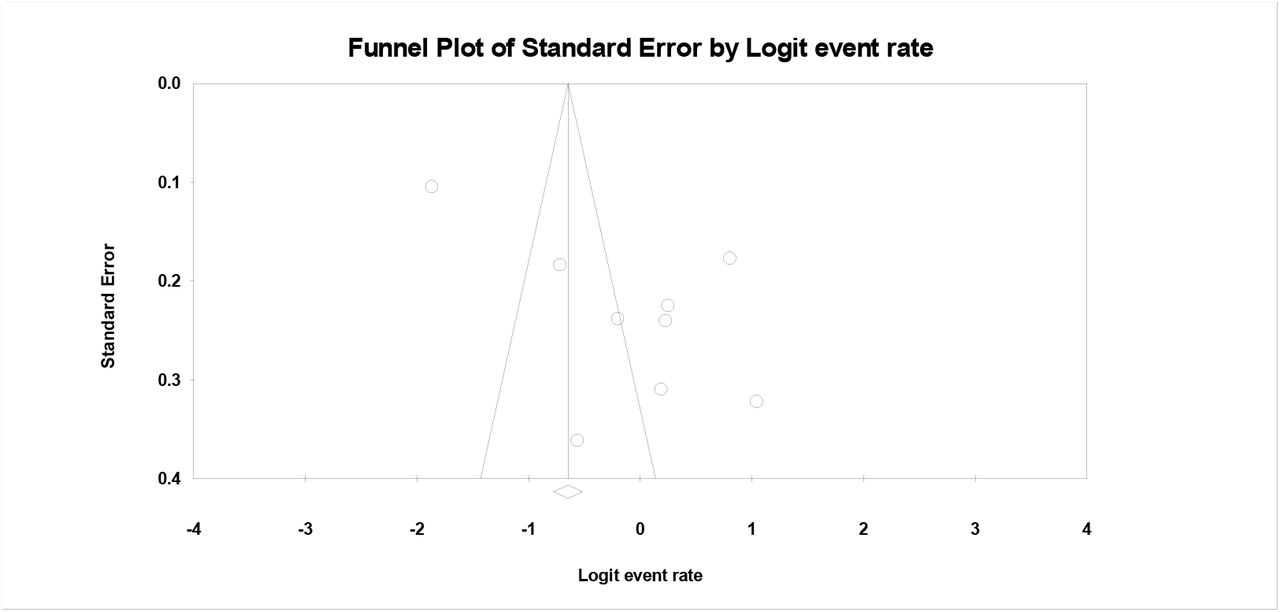
Begg’s and Egger’s tests and the funnel plot were used for publication bias evaluation. A P-value of less than 0.05 was considered as statistically significant.
Results
Study selection process
The first search through databases resulted in 1030 papers. After removing duplicated papers and first step screening based on title and abstract, 89 papers were assessed for eligibility. Finally, 16 articles were entered into the meta-analysis. PRISMA flow diagram for the study selection process is presented in Figure 1.

Study characteristics
Among the 16 studies included in the meta-analysis, all were designed in retrospective nature, except for one study in prospective nature. The studies’ sample size ranged from 10 to 2903, including 4922 participants. Characteristics of studies entered into the systematic review presented in Table 1.
Characteristics of studies entered into the systematic review
Quality assessment
Results of quality assessment for studies entered into meta-analysis based on a modified version of the NOS tool for cross-sectional studies were fair.
Publication bias
Begg’s and Egger’s tests in effect size meta-analysis showed non-significant and significant publication bias for vitamin D status (PB=0.75; PE=0.02, respectively). The funnel plot for publication bias of studies presented in Fig. 2.
Meta-analysis findings
Frequency of Vitamin D status in COVID-19 patients
The meta-analysis of event rates in peer reviewed papers showed that 48% of COVID-19 patients were suffering from vitamin D deficiency (95% CI, 29%-67%), and in 41% of patients, levels of vitamin D were lower than the normal range (95% CI, 10%-82%) (Fig. 3). To maximize the use of everything that exists, the inclusion of pre-prints data to the meta-analysis resulted in a 48% (95% CI, 33%-63%) deficiency and 29% (95% CI, 8%-65%) insufficiency in vitamin D status (Supplementary Fig. 1).

Mean serum 25-hydroxyvitamin D concentration
The meta-analysis of mean 25(OH)D concentration was 18 ng/mL among all COVID-19 patients (95% CI, 13-24), 18.20 ng/mL in severe cases (95% CI, 1-35) and 26 ng/mL in non-severe cases (95% CI, 23.89-28.70) (Fig. 4). Also, by including pre-prints, meta-analysis resulted in 20 ng/mL 25(OH)D in all cases, 18 ng/mL and 26 ng/mL in non-severe and severe cases, respectively (Supplementary Fig. 2).


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
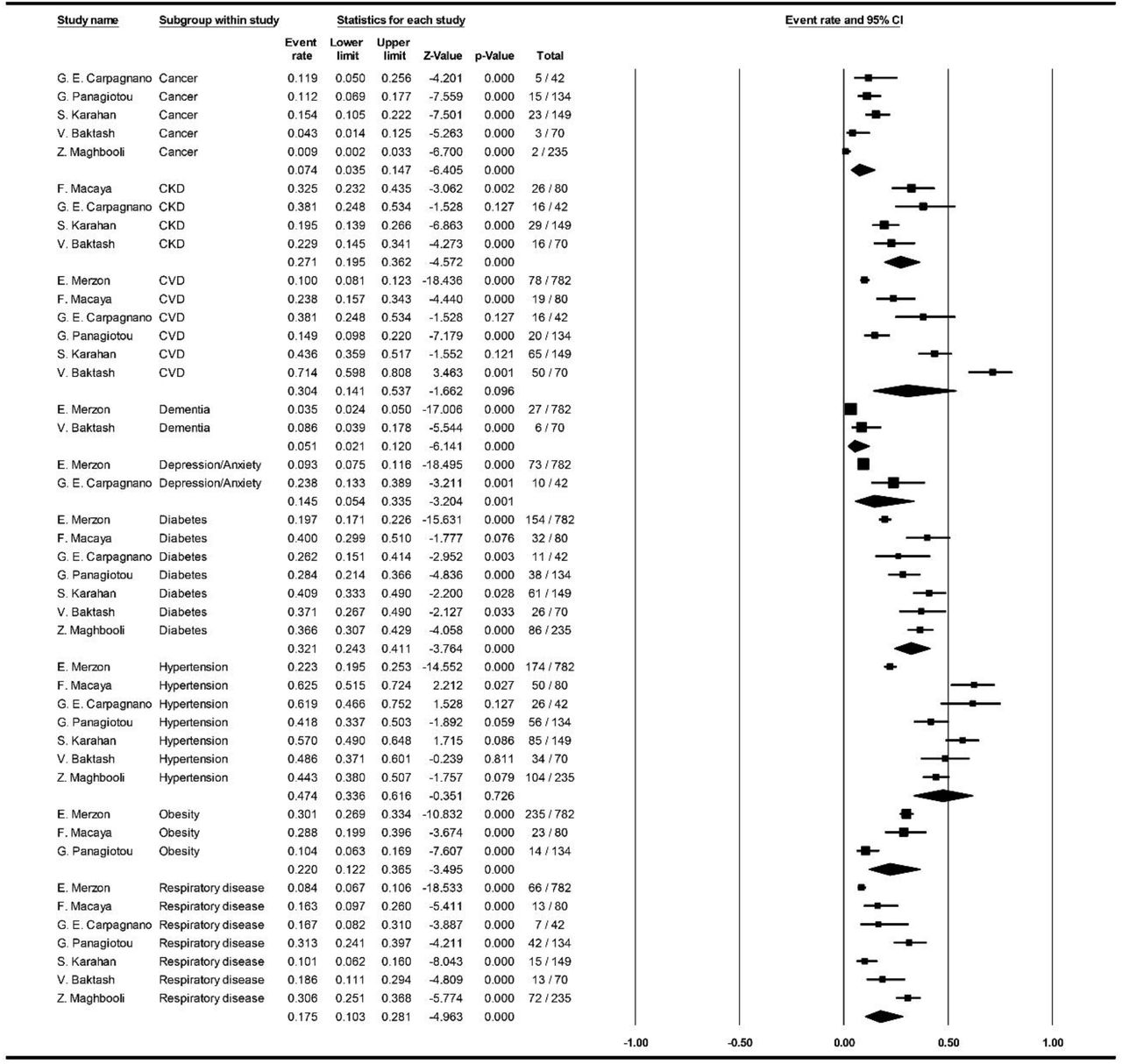
Co-morbidities
Meta-analysis of available data on co-morbidities frequency in COVID-19 patients were as follows: in non-severe cases, 13.0% cancer, 11.8% chronic kidney disease (CKD), 15.4% cardiovascular diseases (CVD), 30.3% diabetes and 35.7% hypertension (HTN), 12.9% obesity, and 18.3% respiratory diseases (Supplementary Figures 3); in severe cases, 12.6% cancer, 34.2% CKD, 30.4% CVD, 41.9% diabetes and 72.6% HTN, 26.4% obesity, and 17.4% respiratory diseases (Supplementary Figures 4); in overall, 7.4% cancer, 27.1% CKD, 30.4% CVD, 5.1% dementia, 14.5% depression/anxiety, 32.1% diabetes, 47.4% HTN, 22.0% obesity and 17.5% respiratory diseases. Frequency of co-morbidities by including pre-prints is presented in Supplementary Figures 5 to 7.
Ethnicity frequency
Pooling available data regarding ethnicity distribution among COVID-19 patients resulted in 1.0% Afro-Caribbean, 10.3% Asian, and 92.1% Caucasian.
Discussion
Epidemiological & clinical aspects
Although comparing global statistics of COVID-19 outcomes is difficult, it is clear that the mortality rate is higher in several countries. It seems that among various factors such as age, healthcare system quality, general health status, socioeconomic status, etc. One of the underestimated factors that might be associated with COVID-19 outcome is the vitamin D status in every population. In recent years, vitamin D deficiency/insufficiency has become a global health issue, and its impact has been studied on respiratory viral infections. Most of the epidemiological studies have been reported a higher risk of developing the infection to the severe stages and death in patients with low levels of vitamin D (24-27). Besides, vitamin D clinical interventions have demonstrated a significantly reduced risk of respiratory tract infection (RTI), further proposed as a prophylactic or treatment approach against RTIs by WHO in 2017 (28-30).
Concerning all of the limitations and lack of high-quality data about the relation of vitamin D status and COVID-19 after several months, we have conducted this systematic review and meta-analysis to maximize the use of every available data, which would give us an overview toward further studies like what we have done recently on the effectiveness of hydroxychloroquine in COVID-19 patients (31), which have underestimated first, but the value was revealed after a while.
According to available data entered into our meta-analysis, we could find that approximately half of the patients infected with SARS-CoV-2 were suffering from vitamin D deficiency, and this vitamin was insufficient in about 41% of them. We have also found that mean 25(OH)D levels were low (<20 ng/mL) in all COVID-19 patients. These findings are in the same line with studies that have debated the association of vitamin D and COVID-19 (32-36). Recently, Kaufman et al. (37), studied the relation of SARS-CoV-2 positivity rates with circulation 25(OH)D among 191,779 patients retrospectively. They found the highest SARS-CoV-2 positivity rate among patients with vitamin D deficiency (12.5%, 95% CI, 12.2-12.8%). Overall, the study indicated a significant inverse relation between SARS-CoV-2 positivity and circulating 25(OH)D levels in COVID-19 patients.
Along with all observational studies, a pilot randomized clinical trial performed by Castillo et al. (38) on 76 hospitalized COVID-19 patients indicated a promising result for calcifediol therapy in these individuals. In this study, high dose oral calcifediol significantly reduced the need for intensive care unit (ICU) treatment. However, due to the small sample size, more extensive, well-organized clinical trials are needed to robust and confirm this study’s findings.
Additionally, in the case of vitamin D supplements’ benefits against acute respiratory tract infections, Martineau et al. conducted a meta-analysis of randomized controlled on 10.933 participants and resulted in an inverse association between vitamin D levels and risk of acute respiratory tract infections. Thus, it can be concluded that patients with lower vitamin D levels or patients with vitamin D deficiency are at higher risk of developing the disease to the severe form (28).
Co-morbidities
After months of investigation on COVID-19, several factors such as male sex, older age, CVD, HTN, chronic lung disease, obesity, and CKD are proposed to be risk factors toward deteriorating COVID-19 patients’ outcomes (39-41). Interestingly, one of the conditions that lead to most of the considered risk factors is vitamin D deficiency. Studies indicated that malignancies, diabetes, HTN, and CVDs are significantly related to vitamin D deficiency. Also, studies reported the important role of vitamin D deficiency in older males (42-44). Evidence shows that aging, physical activity, obesity, seasonal variation, less vitamin D absorption, pregnancy, thyroid disorders, prolonged use of corticosteroids, ethnicity/race can substantially affect the circulating 25(OH)D levels (45-51).
Hence, although studies reported vitamin D deficiency as one of the critical risk factors in clinical outcomes of COVID-19 patients, it seems that it can also be in a strong relationship with basic underlying risk factors and diseases in such patients.
In this case, our analyses indicated that HTN, CVDs, CKDs, diabetes, obesity, and respiratory diseases were the most frequent co-morbidities in COVID-19 patients. According to the facts mentioned above and our findings, it is plausible that both vitamin D deficiency and underlying diseases, which affect each other, may worsen the condition of these patients more than others.
Ethnicity
From the beginning of the COVID-19 pandemic, different studies have been reported probable associations between COVID-19 and the ethnicity of these patients. Most studies found that the mortality rate among black people is higher than the other ethnic groups (52-56). However, other challenges such as human resources, health care systems budgetary, poor management, etc. have to be considered among such people and low-income countries (57-59), which unavoidably affects the subject significantly. In recent years, many studies have focused on vitamin D mechanisms and status among various ethnic groups to find the roles of vitamin D and its relationships with any factors or disorders in various ethnicities (60-63).
Herein, our findings demonstrated that the most frequent ethnic group has belonged to Caucasians, followed by Asian and Afro-Caribbean. Although there is some evidence on the role of genetic variants in COVID-19 patients, the subject is still not clear enough (64, 65).
In contrast to many studies about vitamin D status in different ethnicities, Aloia et al. have reported that serum 25(OH)D concentration is the same in cross-racial comparison. They found an inconsistency between monoclonal and polyclonal assays for detecting vitamin D binding protein (66). Hence, the approach for considering serum 25(OH)D concentration is much important.
Vitamin D mechanisms & COVID-19
Vitamin D metabolism has been well studied throughout history. Numerous investigations indicate vitamin D’s roles in reducing microbial infections through a physical barrier, natural immunity, and adaptive immunity (2, 67-72). For example, investigations on respiratory infections indicated that 25(OH)D could effectively induce the host defense peptides against bacterial or viral agents. Vitamin D insufficiency/deficiency can lead to non-communicable and infectious diseases (2, 73, 74). The other potential role of vitamin D is reducing inflammatory induced following SARS-CoV-2 infection by suppressing inflammatory cytokines, reducing leukocytes’ infiltration, interaction with polymorphonuclear leukocytes, and inhibiting complement component C3 (24, 75-79). Also, according to the available evidence for infections and malignancies (80, 81), vitamin D may enhance the serological response and CD8+ T lymphocytes performance against COVID-19 when the T cells’ exhaustion is related to the critical stages of the disease (82-84).
Besides, according to the revealed association of SARS-CoV-2 and angiotensin-converting enzyme 2 (ACE2), this virus can substantially downregulate the ACE2 expression, which seems to leads the COVID-19 patients to deterioration (85-87). In contrast, vitamin D affects the renin-angiotensin system pathway and promotes the expression of ACE2 (88, 89). However, since the high expression of ACE2 can be a risk factor for the severity of the disease (90), it is not yet clear enough to conclude how much vitamin D helps the condition. Hence, more evidence and trials are needed to design a treatment plan for three groups of mild, moderate, and severe patients.
It is worth noticing that the current meta-analysis includes the following limitations:1) studies entered into the meta-analysis were observational and cross-sectional; 2) There are inevitable challenges with the reliability of data due to different strategies in a testing (e.g., vitamin D measurement, COVID-19 test, etc.), various subpopulations, etc.; 3) other immunomodulatory factors (e.g., vitamin C, zinc, selenium, etc.), which might be influential in the outcome of COVID-19 patients, have not considered in included studies; and 4) type II statistical errors following studies with small sample size. Eventually, to overcome the limitations and bias, the study’s results should be confirmed by robustly large multicentral randomized clinical trials.
Conclusion
The conditional evidence recommends that vitamin D might be a critical supportive agent for the immune system, mainly in cytokine response regulation against pathogens. In this systematic review and meta-analysis, we found that mean serum 25(OH)D level was low (<20 ng/mL) in all COVID-19 patients and most of them were suffering from vitamin D deficiency/insufficiency. The Caucasian was the dominant ethnic group, and the most frequent co-morbidities in COVID-19 patients were HTN, CVDs, CKDs, diabetes, obesity, and respiratory diseases, which might be affected by vitamin D deficiency directly or indirectly. However, further large clinical trials following comprehensive meta-analysis should be taken into account to achieve more reliable findings.
Data Availability
N/A
Conflict of interests
The authors declare that they have no conflict of interests.
Funding
None.
Acknowledgments
We would like to express our appreciation to the Student Research Committee of Mazandaran University of Medical Sciences for approving this student research proposal with the code 7904.
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.
- 6.↵
- 7.↵
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.
- 21.
- 22.
- 23.
- 24.↵
- 25.
- 26.
- 27.↵
- 28.↵
- 29.
- 30.↵
- 31.↵
- 32.↵
- 33.
- 34.
- 35.
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.
- 41.↵
- 42.↵
- 43.
- 44.↵
- 45.↵
- 46.
- 47.
- 48.
- 49.
- 50.
- 51.↵
- 52.↵
- 53.
- 54.
- 55.
- 56.↵
- 57.↵
- 58.
- 59.↵
- 60.↵
- 61.
- 62.
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.
- 69.
- 70.
- 71.
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.
- 77.
- 78.
- 79.↵
- 80.↵
- 81.↵
- 82.↵
- 83.
- 84.↵
- 85.↵
- 86.
- 87.↵
- 88.↵
- 89.↵
- 90.↵




