
Abstract
Objectives To determine if specific ethnic groups are at higher risk of mortality from COVID19 infection.
Design Retrospective cohort study
Setting University Hospitals Birmingham NHS Foundation Trust (UHB) in Birmingham, UK
Participants Patients with confirmed SARS-CoV-2 infection requiring admission to UHB between 10th March 2020 and 17th April 2020
Exposure Ethnicity
Main outcome measures Standardised Admission Ratio (SAR) and Standardised Mortality Ratio (SMR) for each ethnicity was calculated using observed sex-specific age distributions of COVID-19 admissions/deaths and 2011 census data for Birmingham/Solihull. Hazard Ratio (aHR) for mortality was estimated for each ethnic group with white population as reference group, using Cox proportional hazards model adjusting for age, sex, social deprivation and co-morbidities, and propensity score matching.
Results 2217 patients admitted to UHB with a proven diagnosis of COVID-19 were included. 58.2% were male, 69.5% White and the majority (80.2%) had co-morbidities. 18.5% were of South Asian ethnicity, and these patients were more likely to be younger (median age 61 years vs.77 years), have no co-morbidities (27.8% vs. 16.6%) but a higher prevalence of diabetes mellitus (48.0% vs 28.2%) than White patients. SAR and SMR suggested more admissions and deaths in South Asian patients than would be predicted. South Asian patients were also more likely to present with severe disease despite no delay in presentation since symptom onset. South Asian ethnicity was associated with an increased risk of death; both by Cox regression (Hazard Ratio 1.66 (95%CI 1.32 – 2.10)) after adjusting for age, sex, deprivation and comorbidities and by propensity score matching, (Hazard ratio 1.68 (1.33–2.13), using the same factors but categorising ethnicity into South Asian or not.
Conclusions Current evidence suggests those of South Asian ethnicity may be at risk of worse COVID-19 outcomes, further studies need to establish the underlying mechanistic pathways.
Evidence before Published studies of the evolving COVID-19 pandemic have suggested risk factors for the most severe manifestations of the disease, including increasing age, male sex and co-morbidities, especially hypertension, cardiovascular disease and diabetes. There have been observations suggesting poorer outcomes for patients of some ethnicities, and understanding this has become a global priority.
Added value Although still an emerging picture, initial data from our multi-ethnic cohort suggests there are more admissions from South Asian patients than would be expected based on our population, these patients are admitted with a worse severity of COVID19 related respiratory compromise without a significant delay in presentation and experience a higher level of mortality even when differences in age, sex, deprivation and key comorbidities were taken into account. This was consistently shown using different statistical methods.
Implications South Asian ethnicity may form another ‘at risk’ population from COVID-19. However, further studies are needed to better understand the underlying reasons, in particular any modifiable factors to improve outcomes as well as to refine our understanding and communication around non-modifiable risk factors.
Introduction
Coronavirus disease 2019 (COVID-19) was identified in January 2020 (1) and given its designated name by the World Health Organisation in February, 2020 (2). Initial reports from China and then Italy focused on risk factors that predisposed individuals to severe manifestations of infection, including viral pneumonia and adult respiratory distress syndrome (ARDS) requiring critical care support and death. Chen et al (3) described the characteristics of 799 patients admitted to an isolation ward designated for patients with severe or critical COVID-19 in a hospital in Wuhan, China. The patients that had died at the time of the analysis (representing 14.4% of the total cohort) were on average older, more likely to be male and more likely to have a co-morbidity such as hypertension, diabetes or cardiovascular disease. These results have been echoed by further case series reports from authors in China, Italy and the USA (4-6).
A more recent report from the Centers for Disease Control and Prevention (CDC) in the USA described an early signal of non-Hispanic, Black people being disproportionally affected by COVID-19 hospitalisation (7). In the UK, clinicians were voicing concerns over an apparent increase in severe COVID-19 cases (with viral pneumonia requiring critical care support) in patients from ethnic minority backgrounds. This was also suggested by the Intensive Care National Audit and Research Centre (ICNARC) reports, published on 10th April 2020 (8) and 17th April 2020 (9), in which a higher proportion of patients requiring critical care for COVID-19 were of Asian and Black ethnicity compared to pre-COVID historic data (2017 – 2019) for patients who required critical care for viral pneumonia.
It is unclear whether this represents an increased susceptibility to severe disease, or reflects the presence of other factors that have been shown to influence COVID-19 outcome, such as age, social deprivation or the prevalence of co-morbidities that are known to be more common in black and minority ethnic groups (10).
The West Midlands is experiencing a high incidence of COVID-19 associated hospitalisations. This is particularly marked in Birmingham, which has a higher than average percentage of minority ethnic groups, with the 2011 census reporting the following percentages: South Asian 22.3%, Black 7.8%, Mixed ethnicity 4.1%, Others 2.9% and a lower than average White ethnic group at 63% (11).
University Hospitals Birmingham NHS Foundation Trust (UHB) is one of the largest NHS Trusts in England, providing direct acute services and specialist care across four hospital sites, including 2.2 million patient episodes per year, with 2750 beds and an expanded ITU capacity of up to 250 beds during the COVID-19 pandemic. UHB constitutes four acute hospital sites following organisational merger in 2018. At present the Queen Elizabeth Hospital Birmingham (QEHB) runs a fully electronic healthcare record (EHR) (PICS; Birmingham Systems), while the other three sites currently run mixed electronic and paper healthcare records and a shared primary and secondary care record (Your Care Connected). UHB provides secondary care to a population of 1.3 million in Birmingham and Solihull, provides a full range of tertiary services to the WM region and has co-ordinated provision of the NHS Nightingale Hospital Birmingham.
Within Birmingham there was a clinical suspicion that people of South Asian ethnicity may be presenting with more severe COVID-related disease and having worse outcomes. The combination of a high prevalence of ethnic minority groups within the hospital catchment area, a high number of COVID-19 patients being received and a digitally mature NHS Trust permitted an assessment of outcomes from COVID-19 infections with regard to ethnicity (with a particular focus the large group of South Asian ethnicity), age and co-morbidity.
It was hypothesised that people of South Asian ethnicity may be more susceptible to the most severe manifestations of COVID-19 infection and therefore:
have more admissions than would be expected given the prevalence of different ethnic groups within Birmingham (based on the last census data);
have worse outcomes from hospitalised COVID-19 viral infection than White ethnic group, even once age, sex, deprivation and co-morbidities were accounted for;
have more severe disease on presentation, which could not explained by duration of symptoms.
The study had the following aims.
To identify all COVID-19 confirmed patients admitted to UHB hospital within a determined timeframe.
To determine the expected and observed admission and death rate for each ethnic group given the local population.
To determine whether South Asian ethnicity was associated with poor outcomes following hospitalisation with confirmed COVID-19 infection, after adjustment for potentially confounding factors.
To explore if disease presentation was more severe in patients of South Asian ethnicity and if there was any evidence of a delayed presentation to hospital.
Methods
This retrospective cohort study, using prospectively collected data, was conducted in affiliation with DECOVID, an HRA and London - City & East Research Ethics Committee approved research database (Ethics number 20/HRA/1689).
Study population
All patients with a confirmed positive severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) swab result between 9:00am 10th March 2020 and 16:00 17th April 2020, and who were admitted to UHB at the time of or up to two weeks following their first positive COVID swab test were included. COVID diagnoses were confirmed following a nasopharyngeal and oropharyngeal swab in all cases(12), Swabs were processed in accordance with NHS guidance within UHB NHS laboratories (13).
Data Collection and variable definitions
Patient demographics and clinical data were collected from the EHR and from mandatory datasets within the Trust. Clinician-confirmed co-morbidities were available from the EHR, the depth of which was enhanced by access to a summary primary care record (Your Care Connected) and further enriched with diagnostic codes derived from previous hospital episodes. The EHR encodes diagnoses using NHS Digital SNOMED CT browser(14) alongside and mapped on to ICD-10 codes(15) allowing for the presentation and inclusion of historically entered ICD10 codes. Co-morbidities of interest were defined by those associated with poor outcomes from previous publications (16,17) in order to determine the impact of multi-morbidity(17). The most common clusters of diagnostic categories are listed in Table 1. A simple count of co-morbidities was undertaken to determine the impact of multi-morbidity, as described (17). Patient status after hospital discharge was sought to capture any deaths post discharge prior to the study end date (17th April 2020). English Indices of Deprivation scores were calculated using postcodes from the current data provided by the UK’s Ministry of Housing, Communities and Local Government (2019) Report(18).
Legend. Data is number (percentage) unless otherwise stated. Ethnicity was self-reported or inferred (see Methods). Medical conditions were physician-confirmed and checked against admission and linked primary care notes. Pregnancy was self-reported and confirmed by linked primary care records where needed. English Indices of deprivation were calculated using postcode. Severity was determined by respiratory oxygen requirements, see methods. Subgroup data is provided for those ethnicities that represented more than 5% of the whole population.
Ethnicity was self-reported by the patient or their family members on admission to hospital. Where this information was missing, it was gathered from previous admissions and by reviewing primary and secondary medical records. If this was not available (as was the case in 91 patients), ethnicity was imputed from the modal ethnicity of patients with the same surname in the EHR database where possible, as previously described (19) but remained unavailable in 48 patients (see Table 1 for missing data). Ethnicity was grouped as per national guidelines(20).
Severity of COVID-19 on admission
The physician-determined severity of COVID-19 on first admission was categorised using a pragmatic and locally developed score that made use of baseline physiological assessments and oxygen requirements to identify those on admission to hospital who were in need of urgent critical care assessments for respiratory support, as follows.
Patients were considered to have severe respiratory manifestations of COVID-19 infection; if COVID was suspected and the patient required inspired oxygen ≥ 50% to maintain targeted oxygen saturations (>93% except in the presence of type 2 respiratory failure where the target saturations were 88% - 92%) with respiratory pathology thought driven by COVID-19 illness.
If not severe, patients were considered to have moderate severity respiratory manifestations of COVID-19 infection if COVID was suspected and the patient required inspired oxygen of > 4L/min or inspired oxygen > 28% to maintain target oxygen saturations.
Patients were considered to have mild severity respiratory manifestations of COVID-19 infection if the patient had respiratory symptoms but did not meet the severe or moderate criteria as described above.
Baseline physiological assessments to determine severity of COVID-19 were considered to be those taken within 24 hours either side of the SARS-CoV-2 swab collection time, of which the earliest available measurement was used. Since not all patients were admitted within 24 hours of their SARS-CoV-2 swab test, and since these assessments are only routinely recorded in the EHR system for QEHB patients, baseline severity scores were only available for a subset of the patients (736/2217).
To determine if disease severity on admission reflected duration of illness, medical clerking notes were reviewed to determine the duration of symptoms prior to admission. This was available in only a subset of patients (567/2217).
Outcomes
The primary outcome was death while in hospital or post-discharge until the study end date. For those patients discharged from hospital, primary care records were checked and any patients admitted to hospital with COVID-19 and discharged who had died in the community within the censor period were noted. Those with an on-going admission were censored on the study end date.
Statistics
Baseline Characteristics
Baseline characteristics for the total population and ethnic communities are presented as mean (standard deviation) or median (interquartile range) for continuous variables and as frequency (percentage) for categorical variables. Ethnic groups were compared by age, sex, co-morbidity and severity on presentation.
Standardised Admission Rate and Standardised Mortality Rate by ethnicity
Using the observed sex-specific age distributions of COVID-19 admissions and deaths in UHB and 2011 census data for the Birmingham and Solihull area, the expected numbers of admissions and deaths were estimated for each ethnic category. The ratios of observed to expected numbers were calculated to provide standardised admission ratios (SAR) and standardised mortality ratios (SMR) for each ethnic category and 95% confidence intervals were obtained using the mid-P exact test(21).
Predictors of mortality
The overall effects of age, sex, ethnicity, co-morbidities and admission severity on mortality were tested by univariable analysis. The effect of ethnicity on mortality was then considered adjusting for age, sex, comorbidity counts and deprivation in a multivariable analysis. A Cox proportional hazards model was used to derive adjusted Hazard Ratios (aHR) for mortality, defined as death from any cause after COVID-19. Survival time was calculated as the time between the collection of a sample on clinical suspicion and the date of death or study end date and used for Kaplan-Meier estimates. Multiple parameterisations were tested for patient age, including linear fit, square-root transformation, categorical groupings, and natural cubic splines. Categorical variables were fitted for sex, ethnicity, deprivation score quintiles and number of clinically assessed co-morbidities. The proportional hazards assumption was tested through correlation of the scaled Schoenfeld residuals with survival time, with hypothesis tests for independence (22). Models were then tested using Propensity Score weighting (23) where age, sex, social deprivation index and co-morbidities were matched and ethnicity was treated as a dichotomous variable. Models were fitted in R version 3.6.3 using the survival package and twang package in "r" (www.r-project.org)(24). All p-values are reported exactly and no corrections were made for multiple comparisons unless stated.
Results
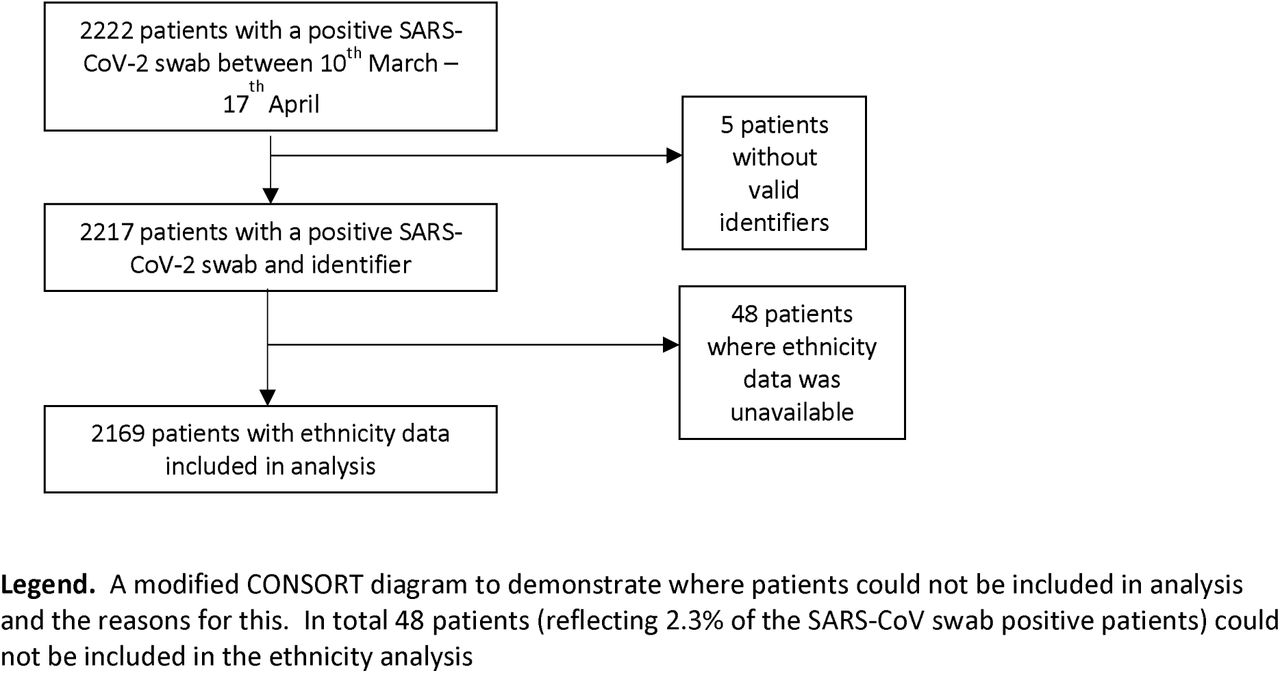
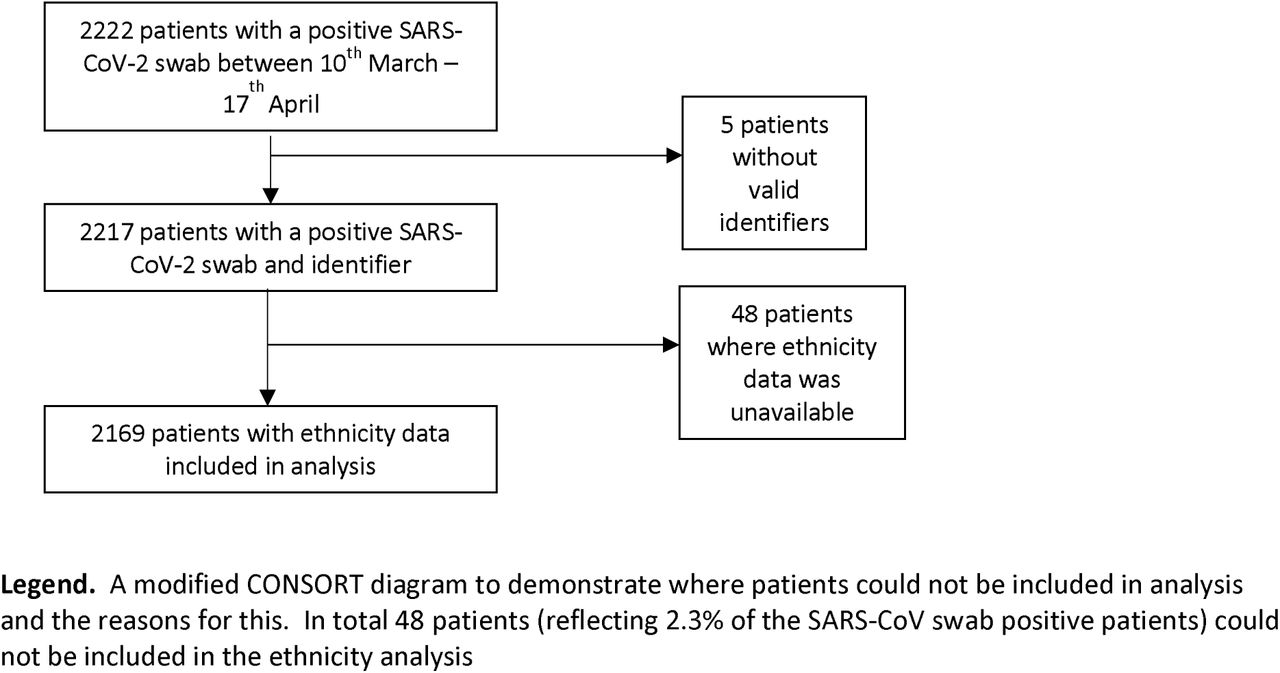
2,217 consecutive patients admitted to UHB with a swab-proven diagnosis of COVID-19 were analysed. A modified CONSORT diagram (Figure S1 of the online supplement) and a summary of the demographic and clinical characteristics on admission (Table 1) are shown. Most patients (n=2132) had a Birmingham postcode. The majority of patients were male (1290/2217; 58.2%) and White (1540/2217; 69.5%). High levels of co-morbidity were identified across all ethnic groups (with 40.1% of patients having three or more co-morbidities).
Of note, up to 50% of patients had missing morbidity data and 30% had missing ethnicity data using secondary care records alone, but >97% of ethnicity data and all available morbidity data was resolved through reviewing primary and secondary care records.
Comparison of baseline characteristics between ethnicities
South Asian patients, when compared to White patients, were younger (median age 61 years vs. 77 years; p<0.001), had a higher prevalence of diabetes mellitus (48.0% vs 28.2%, p<0.001) but lower prevalence of dementia (5.4% vs 18.4%), COPD (4.9% vs 21.6%), atrial fibrillation (6.3% vs 26.2%) and cerebrovascular disease (4.4% vs 15.1%) (p<0.001 for all). Similar to the South Asian patients, Black ethnic patients were younger (median age 62 years), had a higher prevalence of diabetes mellitus (53.7%) but lower prevalence of other key comorbidities than the White population. Two thirds of the South Asian and Black ethnicity came from the most deprived quintile of deprivation compared to 36% from the White patients.
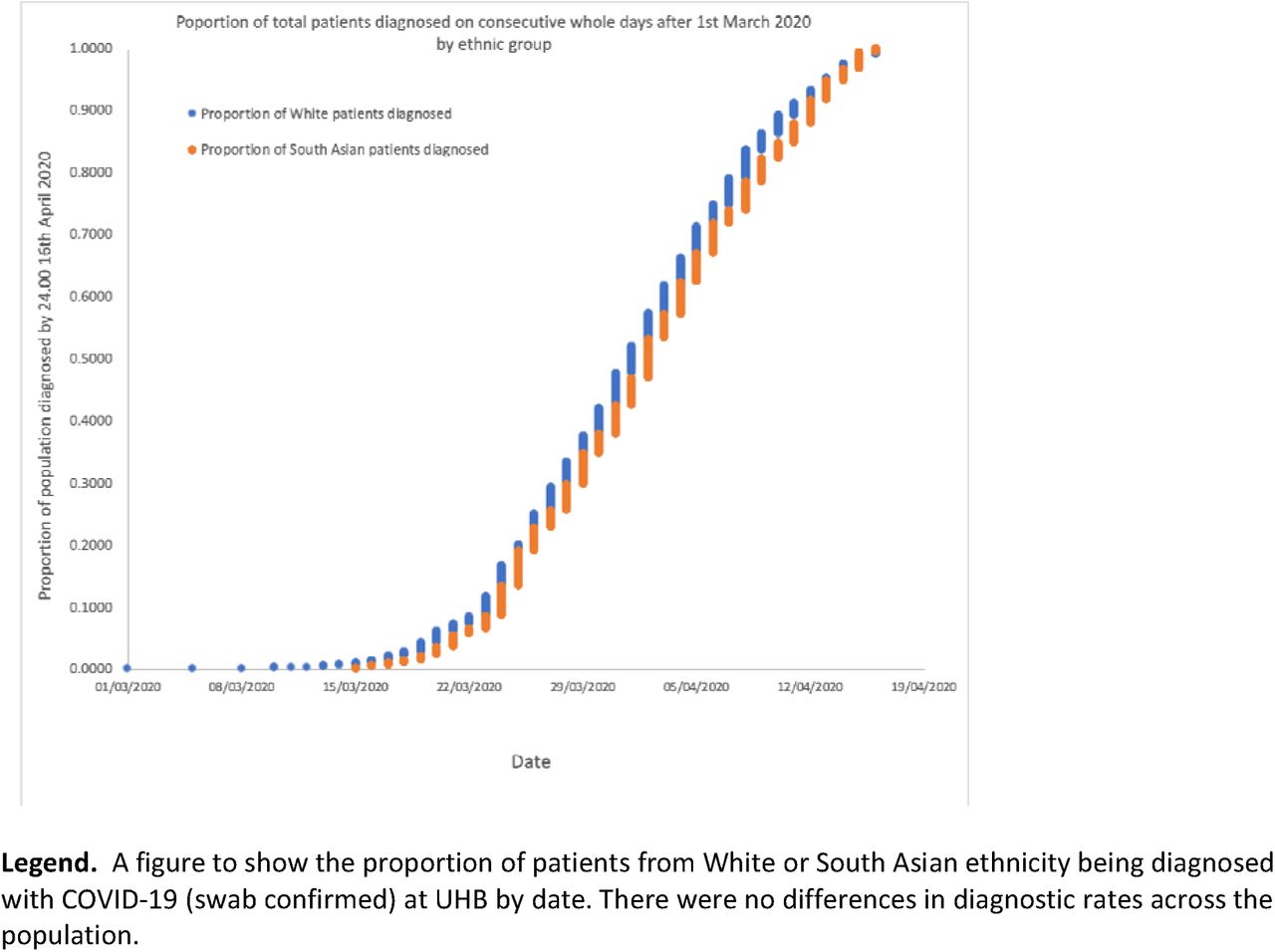
Across the course of data collection, the proportion of patients presenting from different ethnic groups was relatively stable (Figure S2 of the online supplement), suggesting no differential transmission related to ethnic group within the location and timeframe studied.
Standardised Admission Ratio in different ethnicities
Age and sex Standardised Admission Ratio (95% Cl) for South Asian females was 74% higher (SAR, 1.74:95%CI 1.49-2.02) and for South Asian males 63% higher (SAR, 1.63:95%CI 1.44-1.85) than the standard population. (See Table S1 of the online supplement). In contrast, White patients were less likely to be admitted in comparison to the standard population (White females; 0.84 (0.78 – 0.91) and White males; 0.87 (0.81-0.93)). Admission rates were similar to expected rates of the standard population for Black ethnicity.
Severity of COVID19 disease at presentation in different ethnicities
In 736 patients admitted directly to the QEHB site, the severity of COVID-19 recorded on admission identified 185 (25.1%) classified as moderate and 102 (13.9%) classified as severe. In this dataset a higher proportion of South Asians than Whites were assessed to have severe disease on presentation (34/137 (24.8%) vs 54/483 (11.2%) p <0.0001). See table S2 of the online supplement. A higher proportion of South Asians than Whites were admitted to ICU (86/410 (21.0%) vs 133/1540 (8.6%) p <0.001). There were no differences in the duration of symptoms prior to admission by ethnic group ((Median) South Asian = 7 days, White = 6 days, Black =7 days, p=0.40).
Characteristics of patients who died
At the study end date 611/2217 (27.5%) patients had died during the study period. These patients were older, more likely to be male, White, have multiple co-morbidities and in the 736 patients admitted directly to the QEHB site, in whom data was available, more likely to have moderate or severe disease on admission, in comparison to all other groups of patients (table 2).
Legend. Data is number (percentage) unless otherwise stated. Medical conditions were self-reported and checked against admission and linked primary care notes. Pregnancy was self-reported and confirmed by linked primary care records where needed. Groups are compared using Chi-squared analysis, except for pregnancy where Fisher’s exact test was used and age distribution, where Kruskal Wallis was used. Of note, p-values compared all patients currently alive (in patients ordischarged) versus those who had died. * = less deaths in the "Other" ethnicity group (p=0.0001) ** = Increased deaths with 1-2 (p = 0.001) or 3 or more (p<0.0001) co-morbidities on post hoc analysis. *** = increased deaths in moderate and severe cases vs. mild cases on post hoc analysis (p < 0.0001)for comparisons with patients discharged alive and currently alive.
In those in whom data was available, people that died had a shorter duration of symptoms prior to admission compared to those who were still alive (median 4.5 days (2 - 7) vs. 7 (4 - 10) days. In all in whom data was available (567 patients), the duration of symptoms prior to admission did not related to disease severity on admission (p=0.46). The relationships between survival from time of swab collection and age, gender and number of co-morbidities are further illustrated in Figure 1.

Ethnic group outcome analysis
Standardised Mortality Ratio between different ethnic groups
In comparison to the expected number of deaths based on Birmingham and Solihull 2011 census data age and sex structure, there were significantly more South Asian women and men who died with a positive COVID-19 swab than would be expected: Standardised Mortality Ratios (SMR) (95% Cl): Asian females; 2.15 (1.54-2.92): Asian males; 1.94 (1.52 - 2.45). In contrast fewer White women and men died than would be expected: SMR (95% Cl): White females; 0.85 (0.73 – 0.99): White males; 0.88 (0.78-0.98). (See online Supplementary table S1). For those of Black ethnicity, death rates were not different to the expected rates in the standard population.
Survival curves for mortality in different ethnicities
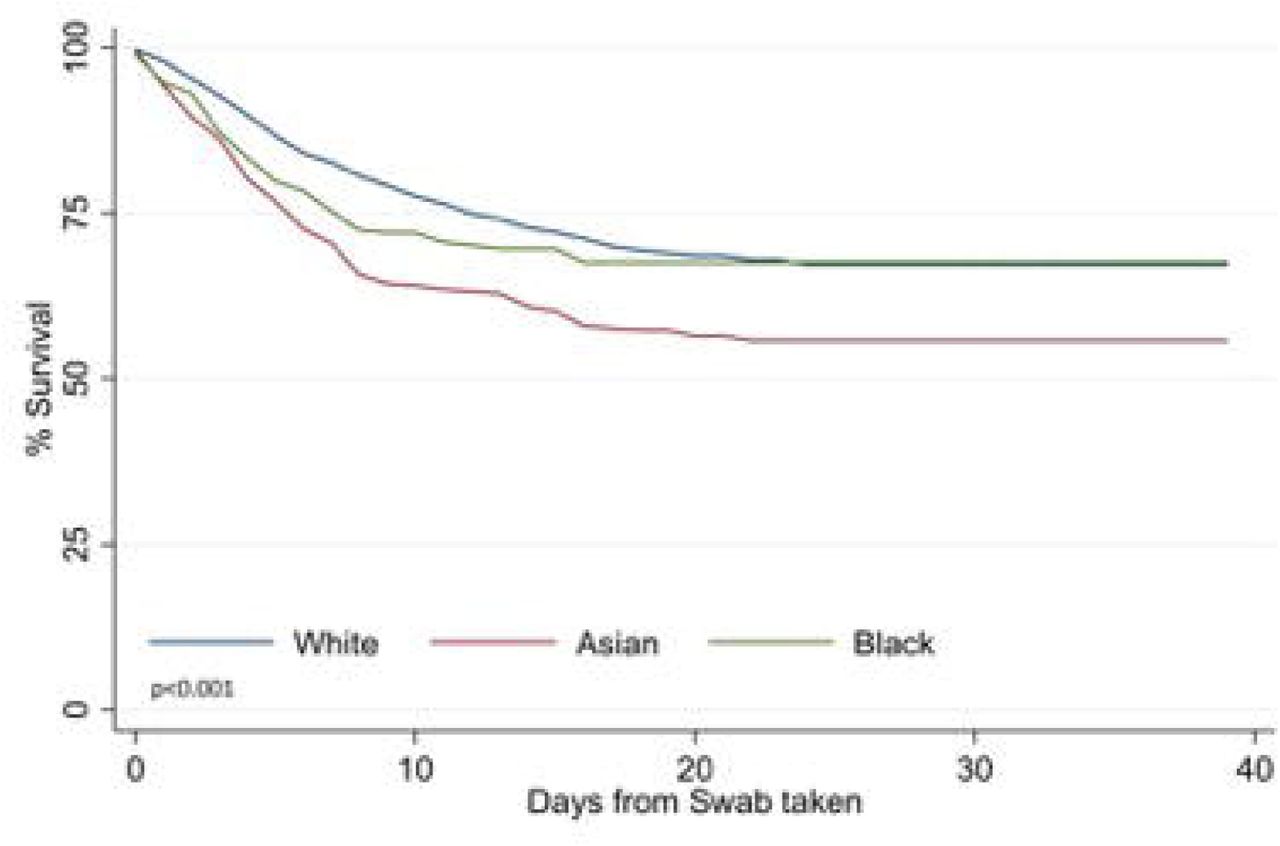
An age-adjusted Kaplan-Meier showed that although there were no differences in age-adjusted survival in White and Black ethnicities, patients from Asian ethnic groups were less likely to survive (See Figure 2).

Legend. Data compares age-adjusted (using categories in Figure 1A) survival status of patients by ethnicity (p <0.001). Comparison using the log-rank test
Multivariable analysis
In a multivariable Cox regression model adjusted for age, sex, comorbidity counts and deprivation, South Asian ethnicity (aHR 1.66, 95%CI: 1.32-2.10) was associated with a significantly higher risk of death. Within the limits of the power of the study there was absence of a significant difference in survival for Black ethnicity compared to the White population (aHR 1.12, 95%CI: 0.78-1.68). In addition to this we found age z-score (aHR 2.80: 95%CI 1.92-4.09) and co-morbidities (1-2 comorbidity, aHR 2.15: 95%CI 1.50-3.09; and 3 or more comorbidities, aHR 3.00: 95%CI 2.09-4.31) as significant predictors. We also found a significant interaction effect between age and sex (aHR for age interaction with male sex, 1.34, 95% Cl: 1.07-1.68), resulting in an amplified risk in males with increasing age (Table 3). The main effects of age and multiple co-morbidities were modified by an interaction (aHR for age interaction with 1-2 comorbidities, 0.76, 95%CI: 0.51-1.12; for age interaction with 3+ comorbidities, 0.51, 95% Cl: 0.34-0.75), that attenuated the relative impact of increasing comorbidity at advanced age.
Multivariable Cox regression model including age (z-score), ethnicity, sex deprivation and comorbidity count as covariates. Adjusted Hazard Ratios along with their confidence intervals are presented.
To further test the assumption that South Asian ethnicity was associated with worse outcomes even when co-morbidities, deprivation, age and sex were considered, propensity score weighting was conducted, matching for the same factors in the Cox regression but categorising ethnicity into South Asian or not. With propensity score weighting the Hazard ratio for risk of death was 1.68 (1.33-2.13) for South Asian patients compared with non-South Asian patients. When co-morbidities were added independently (rather than as a count) using propensity score weighting, South Asian ethnicity was still associated with a significantly higher risk of death (HR 1.50 (95% Cl 1.15-1.96).
Discussion
This is the first study to specifically describe the impact of South Asian ethnicity on the outcome of COVID-19 infection using highly characterised and accurate primary and secondary data from patients admitted to hospital in the UK. South Asians were significantly younger than White patients and, when accounting for the age structure of the local population, had a higher admission rate.
There were high levels of co-morbidity in all affected ethnic groups. However, South Asians exhibited a higher prevalence of diabetes mellitus and lower prevalence of dementia, COPD, cerebrovascular disease and atrial fibrillation when compared to the White ethnic group.
Importantly, after adjusting for age, sex, deprivation, and multiple co-morbidities the effect of South Asian ethnicity on mortality was highly statistically significant when assessed using two recognised techniques: a Cox proportional hazards regression model and propensity score weighting.
The excess age-adjusted mortality in COVID-19 is therefore not solely attributable to a range of cardiovascular and metabolic risk factors that are over-represented in this ethnic group. In sensitivity analysis the Hazard Ratio for South Asian ethnicity using both Cox regression and Propensity score matching was stable when ‘number of co-morbidities’ was exchanged for the presence of specific comorbidities including diabetes mellitus and hypertension. To place this in context, the effect of South Asian ethnicity on mortality is significantly less than the effect of one or more co-morbidities (present in 80.2% of all admitted patients) and approximates to the effect of ageing ten years in the White population. In this study we observed no independent signal related to higher deprivation levels(25) and poor outcomes.
It is notable that in the sub-analysis of patients admitted to QEHB, where we were able to immediately integrate a COVID-19 specific assessment into our electronic healthcare record, South Asian patients appear to present with more severe disease but with no difference in the duration of symptoms prior to admission. These findings could reflect different health service utilisation or disease course in the South Asian population. Indeed, comparing all those still alive and those who had died by the end of the study, patients who died had a shorter history of symptoms prior to admission, consistent with an association between disease course and outcome.
A significantly higher rate of admission to ITU in the South Asian ethnic group could relate to this more severe disease at presentation. It may also relate to patient-level differences in joint decision-making regarding ITU treatment, in patients who have higher levels of specific co-morbidities such as dementia and COPD. These groups are significantly over-represented in the White ethnic group, which was also significantly older.
The limitations in our overall analysis need to be considered, specifically that 25% of patients remain in hospital at the time of the data lock, so our findings will evolve. Since the proportion of patients presenting from different ethnic groups was stable across the course of data collection, any consequence for our main conclusion on the mortality risk in South Asians admitted to hospital is likely to be small.
It is also important to acknowledge that standardised admission and mortality ratios from Birmingham and Solihull use the most recent census data, but that these are from 2011. Estimates of the contemporary age structure do not, however, suggest a need to significantly qualify these findings. The UK has not undertaken widespread screening or diagnosis of patients in the community. We are therefore unable to comment upon the natural history of COVID-19 prior to admission to secondary care. We cannot account for the rate of infection in the community or patient and professional behaviours that influence admission from the community, which may differ between ethnic groups. A description of disease in the community will help build a clearer understanding of the apparent excess mortality following admission, for which there remain a number of possible explanations. A limitation of any observational study is that it is limited by the clinical variables available in the record. However, a real strength in this analysis has been the ability to study a highly curated and complete data set, without the inherent issues of significant undercoding seen with morbidity and ethnicity data when using a secondary care dataset collected on admission.
The biological basis of any difference in outcome following admission can only be speculated upon at present. There are reported differences in outcomes for non-white ethnic groups from ARDS even after adjusting for sex, age, disease severity, type of hospital, and median household income(26, 27). The worst clinical manifestations of COVID-19 appear to be associated with a cytokine storm syndrome. Here a hypercytokinaemia is seen (4), with predictors of mortality reflecting a virally induced inflammatory state which can be assessed using a scoring system including validated clinical laboratory tests (28). Candidate genes associated with ARDS have been identified in bioinformatic analyses with a strong predominance of inflammatory pathways, including reactive oxygen species, innate immunity-related inflammation, and endothelial vascular signalling pathways (29). Ethnicity may influence cytokine gene polymorphisms and inflammatory profiles following specific challenges (30), with some ethnic groups more prone to a heightened inflammatory response. This remains poorly understood and there is an urgent need to understand the genomic and associated phenomic characteristics of patients who are susceptible or resistant to the severe manifestations of COVID-19 to understand this further.
Although our study includes only one NHS Foundation Trust, it covers an ethnically diverse contiguous population of 1.3 million people for which it is the sole provider of adult acute secondary care across four hospital sites. This provides for continuity of data, clinical protocols and access to therapy. The immediate availability of access to an electronic representation of a primary care record to support the care of admitted patients also supports the integrity of data collection, the quality of which might otherwise be more limited (31).
Our findings, which describe and quantify the risk of COVID19 in the South Asian population are relevant to national policy and to understanding the underlying biological mechanisms in ‘at risk’ populations. Future studies will extend our observations and explore underlying epidemiology and biological mechanisms; to improve interventions based in the community, the emergency department, ward and ITU. Perhaps most importantly our findings inform the UK’s national discussion on at ‘at risk’ groups and the ensuing fear arising from uncertainty.
Data Availability
To facilitate knowledge in this area, the anonymised participant data and a data dictionary defining each field will be available to others through application to DECOVID via the corresponding author. The data will be available upon request and following approval of a process to ensure ethical data governance and through a data access agreement. Please contact the corresponding author for details.
Data Sharing Agreement
To facilitate knowledge in this area, the anonymised participant data and a data dictionary defining each field will be available to others through application to DECOVID via the corresponding author. The data will be available upon request and following approval of a process to ensure ethical data governance and through a data access agreement. Please contact the corresponding author for details.
Author contribution
E Sapey designed the study, collated data, performed some analysis, wrote the manuscript. S Gallier collated data, performed analysis, wrote the manuscript. C Mainey performed statistical analysis. P Nightingale performed statistical analysis and helped write the manuscript. D McNulty performed statistical analysis. H Crothers performed statistical analysis. F Evison performed statistical analysis. K Reeves performed statistical analysis. D Pagano assisted with the design of the study and manuscript preparation. P Diggle assisted with analysis. K Nirantharakumar and AK Denniston assisted with analysis and manuscript writing. S Ball designed the study, oversaw data collection and helped write the manuscript. All authors amended the manuscript and approved the final version. The data was curated and analysed on behalf of all clinicians at UHB.
Copyright
The Corresponding Author has the right to grant on behalf of all authors and does grant on behalf of all authors, an exclusive licence (or non-exclusive for government employees) on a worldwide basis to the BMJ Publishing Group Ltd to permit this article (if accepted) to be published in BMJ editions and any other BMJPGL products and sub-licences such use and exploit all subsidiary rights, as set out in our licence.
Transparency declaration
E Sapey (the manuscript’s guarantor) affirms that the manuscript is an honest, accurate, and transparent account of the study being reported; that no important aspects of the study have been omitted; and that any discrepancies from the study as planned (and, if relevant, registered) have been explained.
This study was approved by HRA and London - City & East Research Ethics Committee approved research database (Ethics number 20/HRA/1689)
The study was funded by Health Data Research UK as part of PIONEER but the funder did not direct or contribute to any research outputs and researchers developed, conducted and wrote up this report independent to the funder
The study was sponsored by University Hospital Birmingham NHS Foundation Trust
Patients and public members were consulted as to the use of health data to improve the care for people with acute, unplanned illness and a group of patients recovering from COVID-19 specifically support the use of health data to investigate the relationship between poor outcomes and ethnicity.
Conflicts of Interest
S Gallier, C Mainey, P Nightingale, D McNulty, H Crothers, F Evison, D Pagano’ report no conflicts of interest. S Ball and P Diggle reports funding support from HDRUK, K Reeves reports funding support from the NIHR, E Sapey reports funding support from HDRUK, MRC, Wellcome Trust, NIHR and British Lung Foundation. K Nirantharakumar reports funding from MRC, Wellcome Trust, NIHR, Vifor and AstraZeneca. AK Denniston reports funding from HDRUK, Wellcome Trust and Fight for Sight.
Online Supplement

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Acknowledgements
This work was supported by Health Data Research UK (HDRUK), an initiative funded by UK Research and Innovation, Department of Health and Social Care (England) and the devolved administrations, and leading medical research charities. This work uses data provided by patients and collected by the NHS as part of their care and support. We would like to acknowledge the contribution of all staff, key workers, patients and the community who have supported our hospitals and the wider NHS at this time
The manuscript was prepared and submitted on behalf of all of the staff at UHB NHS Foundation Trust
With particular thanks to
Medical Students: Lylah Irshad, Maxim Harris, Theodore Nabavi,
Health Informatics: A Kolesnyk, M Ahmed A Liaqat
Tanya Pankhurst, Jamie Coleman, Chirag Dave, Khaled ElFandi, Rifat Rashid, Paul Cockwell
DECOVID partners include UHB, University of Birmingham, University College London Hospital, University College London, Alan Turing Institute and this dataset will be available through DECOVID (see www.DECOVID.org).
References




