
Abstract
Background and Objective Since the outbreak of coronavirus disease 2019 (COVID-19) in December 2019 in Wuhan, Hubei Province, China, it has spread around the world and become a global public health emergency. It is important to distinguish COVID-19 from other viral pneumonias in order to properly screen and diagnose patients, reduce nosocomial infections, and complement the inadequacy of nucleic acid testing. In this study, we retrospectively analysed the clinical data of COVID-19 versus non-COVID-19 patients treated at our hospital between January 17 and February 27, 2020 in order to summarize our clinical experience in the differential diagnosis of COVID-19.
Methods In this retrospective cohort study, 23 confirmed COVID-19 patients were consecutively enrolled from January 17 to February 27, 2020, while 29 confirmed non-COVID-19 patients were enrolled in West China Hospital of Sichuan University. We collected baseline data, epidemiological data, clinical characteristics, imaging findings, viral nucleic acid test results, and survival data. SPSS v22.0 was used for statistical analysis. Outcomes were followed up until March 25.
Results A total of 52 patientswere included in this study, including 23 COVID-19 patients and 29 non-COVID-19 patients. No significant between-group difference was observed inage, sex, primary signs orsymptoms, cellular immunity, or platelet count. Significant between-group differences were observed in clinical characteristics such as dry cough, contact with individuals from Wuhan, some underlying diseases, nucleated cell count, chest imaging findings, viral nucleic acid test result, 28-day mortality, and 28-day survival.
Conclusion Epidemiological data, clinical symptoms, nucleic acid test results for COVID-19 and chest CT manifestation may help distinguish COVID-19 from non-COVID-19 cases, prevent imported cases and nosocomial infections.
Introduction
Coronavirus disease 2019 (COVID-19) was first detected in December 2019 in Wuhan, Hubei Province, China[1]. The virus spread to other regions of China via human-to-human transmission[2, 3], resulting in imported cases and clusters of cases. Since then, COVID-19 has spread rapidly around the world. As of March 31, 700 000 confirmed cases had been reported worldwide. The outbreak occurred along with seasonal infections, such as influenza and other transmissible viral respiratory diseases[4]. Therefore, it is important to distinguish different types of viral pneumonia. Given the rapid spread of COVID-19 and its significant impact on public health[5, 6], some researchers have collected data from different hospitals and investigated the clinical characteristics of COVID-19 versus bacterial pneumonia[7]. However, the researchers did not compare COVID-19 and other viral pneumonia that occurred during the same period. COVID-19 is highly contagious[6, 8, 9] and spreads quickly [10, 11] without apparent symptoms in some cases [12, 13]. Nucleic acid testing is currently the main method of diagnosis[14]. Early nucleic acid testing plays a key role in detecting patients early and facilitating their early quarantine and treatment[15]. However, nucleic acid testing has some limitations, including a high false-negative rate[16] and variation in the quality of reagents from different sources. Epidemiological data, chest imaging findings, and clinical characteristics must be taken into consideration to make a diagnosis. It is important to distinguish COVID-19 and other viral pneumonia in order to properly screen and diagnose patients and reduce nosocomial infections. In this study, we retrospectively analysed the clinical data of COVID-19 versus non-COVID-19 patients treated at our hospital between January 17 and February 27, 2020 in order to provide a reference for the differential diagnosis of COVID-19, help evaluatethe prevention and control of nosocomial infections at our hospital, and add to the published clinical experience.
Methods
Ethicsreview
This retrospective study was approved by the Ethics Committee of West China Hospital, Sichuan University, on February 10, 2020(EC Number:2019 No.130).
Data collection
We searched electronic medical records in the medical information database of our hospital with the following keywords: unexplained fever, severe acute respiratory syndrome, coronavirus 2 (SARS-CoV-2), viral pneumonia, respiratory infection, bronchitis, pulmonary infection, pneumonia, severe pneumonia, and acute respiratory distress syndrome (ARDS). We retrieved and retrospectively analysed case data (per patient ID), including the baseline data, epidemiological data, clinical characteristics, laboratory test results, imaging findings, and results of the nucleic acid test for SARS-CoV-2. The data were entered in a standardized data collection form and then independently reviewed by two investigators to check the data accuracy and the availability of epidemiological data and information about clinical symptoms. In case of missing data, the investigators contacted the attending physicians and patients or their families directly to obtain accurate data.
Sample collection for virus tests and chest computed tomography (CT)
A throat swab or broncho alveolar lavage fluid was collected according to the standard sampling requirements and procedures from all patients admitted to West China Hospital, Sichuan University, between January 17 and February 27. The samples were sealed and sent to the clinical laboratory for screening of 11 viruses (influenza A virus, adenovirus, bocavirus, rhinovirus, influenza A virus subtype H1N1, parainfluenza virus, metapneumovirus, influenza B virus, influenza A virus subtype H3N2, coronavirus, respiratory syncytial virus) and for the nucleic acid test for SARS-CoV-2. Moreover, all patients underwent chest CT.
The inclusion criteria and exclusion criteria are shown in the study protocol (Figure 1). Baseline data were collected, including age, sex, underlying diseases, and history of travelling to or from Wuhan or contact with individuals from Hubei. Clinical symptoms included cough, fever, difficulty breathing, chest pain, chest tightness, headache, muscle aches, fatigue, and diarrhoea. Laboratory tests included white blood cell count (WBC), neutrophil countand percentage, lymphocyte count, cellular immunity(CD4:CD8 ratio), platelet count, procalcitonin (PCT), alanine aminotransferase (ALT), lactate dehydrogenase (LDH), and creatinine (Cr). Moreover, chest imaging findings, viral nucleic acid test results, 28-day mortality, and 28-day survival were collected. We analysed and compared these data in COVID-19 versus non-COVID-19 patients.

Flow chart of study enrolment
Statistical analysis
Pearson’s chi-squared test or Fisher’s exact probability method was used to comparecount data between groups. Normally distributed data areexpressed as the mean±standard deviation. One-way ANOVA or Student’s t-test was used for measurement data. Non-normal data were compared using the Wilcoxon rank-sum test. The 28-day mortality test was conducted using log-rank Kaplan-Meier analysis of the logarithmic survival curve.P values less than 0.05 indicated statistical significance. The statistical tool used was SPSS 22.0 (SPSS Science Inc., Chicago, IL, USA).
Results
We searched the medical information database of our hospital with relevant keywords and retrieved 157 cases treated at our hospital between January 17and February 27. Among them, 52 patients were diagnosed with viral pneumonia based on positive nucleic acid test results and chest CT and thus met the inclusion and exclusion criteria of this study. Specifically, 23patients (44.23%) were diagnosed with COVID-19. Among them, one patient also had parainfluenza virus infection, and one patient also hadinfluenzaA/B virus infection. All COVID-19 patients were admitted to the isolation ward of the Department of Infectious Diseases. During the same period, 29 patients (55.77%) diagnosed with other viral pneumonias (non-COVID-19) were admitted to our hospital. Among them, 12 patients had cytomegalovirus infection, eight had influenza A (H3N2) infection, four had rhinovirus infection, four had Epstein-Barr virus infection, three had respiratory syncytial virus infection, one patient had influenza B infection, one patient had adenovirus infection, and one patient had metapneumo virus infection. All of these cases were common viral respiratory infections in winter.
No significant between-group difference was observed in age, sex, fever, muscle aches, fatigue, headache, chest pain, diarrhoea, heart rate, blood pressure, respiratory rate, cellular immunity, platelet count, ALT, or liver or kidney function (Table 1). Significant between-group differences were observed in dry cough, difficulty breathing, history of travelling to or from Wuhan, history of contact with individuals from Hubei, some underlying diseases, viral nucleic acid test result, WBC, neutrophil count and percentage, lymphocyte count, PCT, Intensive Care Unit (ICU) admission rate, 28-day mortality, and 28-day survival (Table 1).
Demographics and baseline characteristics of COVID and non-COVID patients
Laboratory findings of COVID and non-COVID patients on admission to hospital
Discussion
Within 3 months of the first COVID-19 report in Wuhan, more than onemillion confirmed cases have been reported worldwide. Thanks to effective prevention and control measures implemented during the first 50 days in China[17], the basic reproduction number (R0) of the SARS-CoV-2 has been suppressed from 3.15 on January 23 to 0.04, preventing at least 700 000 cases outside Wuhan. COVID-19 occurred during the peak season for other viral respiratory infections, including viral pneumonia[18]. Therefore, it is important to distinguish COVID-19 from non-COVID-19 cases. In this study, we analysed the clinical data of patients with viral pneumonia treated at our hospital during a single period and found that all 23 COVID-19 cases were imported cases. At the initial visit, only 69.57% of the patients had fever, and approximately one-third had no fever. Nucleic acid test results may be positive before symptoms appear [19], posing a great challenge for the early detection of imported COVID-19. Dry cough is a typical symptom of COVID-19, which should be noted during inquiry to prevent missed diagnoses. Both COVID-19 and non-COVID-19 were more common in middle-aged adults, as the mean age was 45 in the COVID-19 group and 53 in the non-COVID-19 group. In both groups, two-thirds of the patients were men. These data are consistent with those of large clinical studies[12, 20]. In addition, most COVID-19 patients (91.30%) had a history of travelling to or from Wuhan or contact with individuals from Wuhan [21], while non-COVID-19 patients had no clear history of contact. COVID-19 patients were younger with fewer underlying diseases, while non-COVID-19 patients were older with more underlying diseases (such as cerebrovascular disease, organ transplant, haematological tumour, chronic obstructive pulmonary disease, rheumatic disease, diabetes, and immunodeficiency), more severe conditions, a higher ICU admission rate, and higher 28-day mortality (Table 1). The 28-day survival rate was higher in the COVID-19 group (Figure 2). COVID-19 was more likely to affect T cell immunity, resulting in weakened T cell/cellular immunity. Most COVID-19 cases were mild and presented typical symptoms (such as dry cough with little phlegm). Only three COVID-19 patients were admitted to the ICU.
It is important to figure out how to screen and diagnose COVID-19 early in order to prevent imported nosocomial infections. This study showed that clinical symptoms and blood test may provide important clues. No significant between-group difference was observed in fever, blood pressure, heart rate, respiratory rate, platelet count, or kidney function. In addition to dry cough, COVID-19 was characterized by lower WBC, neutrophil count and percentage, and lymphocyte count and percentage, which, combined with the history of exposure to individuals from Hubei and positive nucleic acid test results, may help diagnose COVID-19. In COVID-19 patients, chest CT showed the following characteristics: 1) in most cases, CT showed typical visceral pleural inflammatory exudate on days 5–7 of onset (Figure 2A, day 6 of onset, ‘inflammation line’, yellow arrow); 2) typical CT findings included multiple hazy, patchy ground glass opacities near the visceral pleura in the middle and lower lobes (Figure 2B, day 10 of onset, red arrow); 3) in mild cases, CT showed small, patchy ground glass opacities without clear boundaries (Figure 2C, day 2 of onset, red arrow);4)in severe cases, chest CT showed bilateral multiple large, patchy ground glass opacities with consolidation (Figure 2D, day 8 of onset, red arrow). Non-COVID-19 was associated with different time of onset, disease course, disease severities, and chest CT findings. In rhinovirus infection combined with influenza B pneumonia, CT showed bilateral scattered patchy opacities and parenchymal bands with bronchiectasis (Figure 2E, day 14 of onset, red arrow). Cytomegalovirus infection combined with fungal, bacterial, or pneumocystis pneumoniais usually seen after organ (Kidney) transplant; in our cytomegalovirus patients, chest CT showed bilateral scattered ground glass opacities with interstitial consolidation (Figure 2F, day 14 of onset, red arrow). In severe influenza A pneumonia, CT showed bilateral diffuse bronchial thickening, with parenchymal bands and consolidation around the bronchi (Figure 2G, day 8 of onset, red arrow). In severe respiratory syncytial virus pneumonia with rheumatoid arthritis, chest CT showed multiple patchy opacities, parenchymal bands, ground glass opacities, consolidation, reticular markings, and interstitial fibrosisin both lungs (Figure 2H, day 10 of onset, red arrow). These characteristics help distinguish COVID-19 and other viral pneumonia[22–26].
Figure 1 shows the flow chart of study enrolment. Significant between-group differences were observed in their clinical characteristics. The28-day survival rate was significantly higher in the COVID-19 group than in the non-COVID-19 group (Figure 2).

Typical visceral pleural inflammatory exudate on days 5–7 of onset (day 6 of onset, ‘inflammation line’, yellow arrow)

multiple hazy, patchy ground glass opacities near the visceral pleura in the middle and lower lobes ( day 10 of onset, red arrow)

small, patchy ground glass opacities without clear boundaries (day 2 of onset, red arrow)

bilateral multiple large, patchy ground glass opacities with consolidation (day 8 of onset, red arrow)

bilateral scattered patchy opacities and parenchymal bands with bronchiectasis (day 14 of onset, red arrow)

bilateral scattered ground glass opacities with interstitial consolidation (day 14 of onset, red arrow)

bilateral diffuse bronchial thickening, with parenchymal bands and consolidation around the bronchi (day 8 of onset, red arrow)
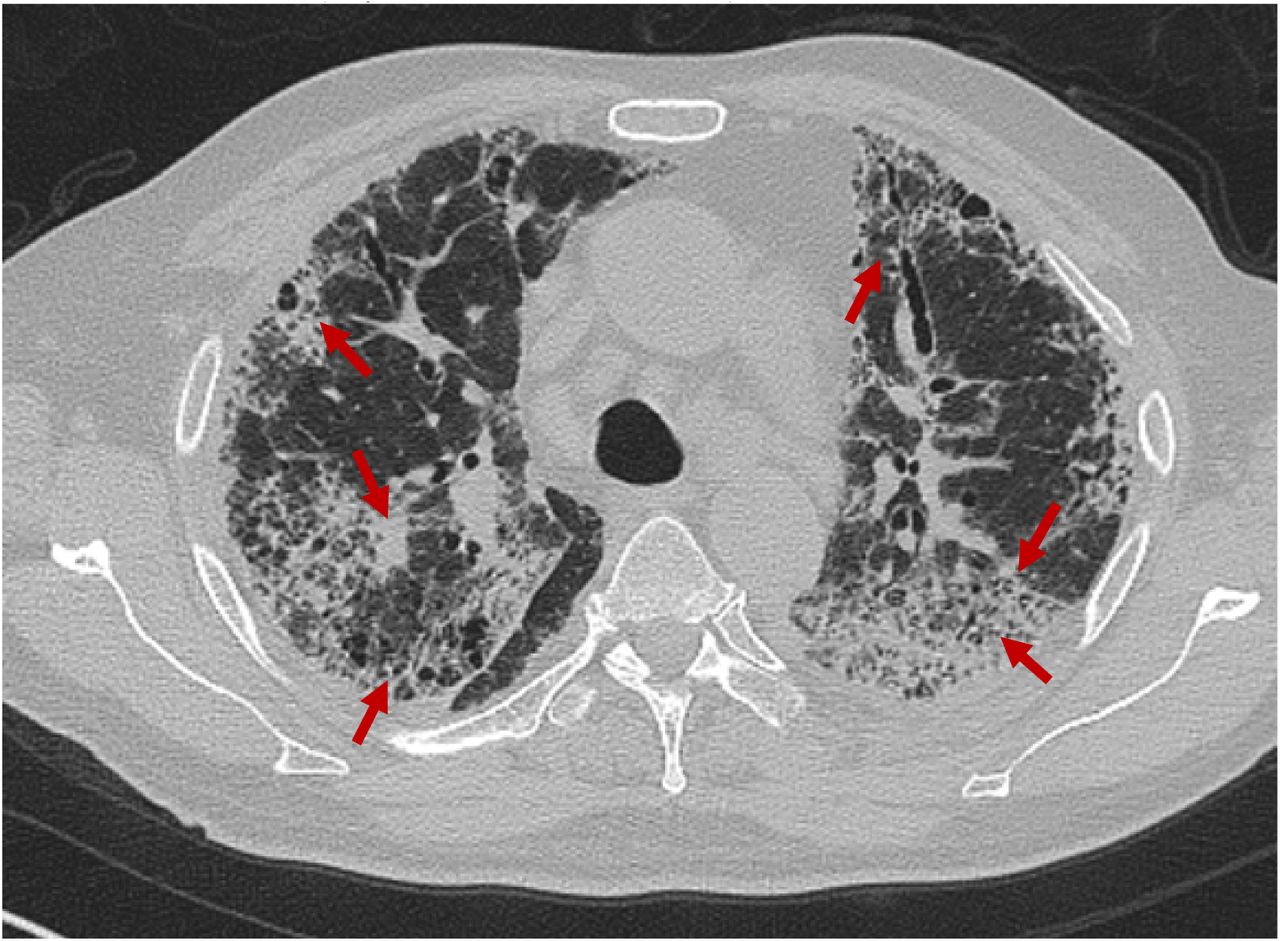
multiple patchy opacities, parenchymal bands, ground glass opacities, consolidation, reticular markings, and interstitial fibrosisin both lungs (day 10 of onset, red arrow)

The 28-day survival rates of CVODI-19 versus non-COVID-19 patients (higher for COVID-19, P = 0.002)
This study has some limitations. First, this was a retrospective study with a short observation time, so the level of evidence was lower than that of prospective randomized controlled trials. Second, the sample size was small, with only 23 COVID-19 cases, furthermore, most of which were mild, and only three patients were admitted to ICU according to our protocol[27]. Non-COVID-19 patients were older with more underlying diseases, which were more critical. 12 of whom were admitted to ICU. The 28-day mortality rate of non-COVID-19 patients was higher than that of COVID-19 patients, and the 28-day survival rate of non-COVID-19 patients was lower than that of COVID-19 patients. Third, no effective treatment is available for COVID-19. We followed the guidelines [28] and administered oxygen therapy, oxygen atomization and humidification, antiviral therapy (lopinavir/ritonavir tablets, Arbidol, interferon nasal spray), ambroxol (to break up phlegm), acetylcysteine (Fluimucil, to prevent pulmonary fibrosis), and live combined Bifidobacterium and Lactobacillus tablets (to supplement intestinal probiotics), as well as a-thymosinfor supportive symptomatic treatment in the case of decreased Tlymphocytes. Other than traditional Chinese medicine (oral or via a nasal tube), the treatment protocol lacks specifics. Lastly, prospective studies are needed to validate our results.
This study shows that history of contact with individuals from Wuhan, dry cough, low WBC, low neutrophil count, low lymphocyte count, low Tlymphocyte count, typical chest CT findings, and a positive nucleic acid test for SARS-CoV-2 help screen and diagnose COVID-19 and distinguish it from other(non-COVID-19)viral pneumonia.
Conclusion
Epidemiological data, clinical symptoms, nucleic acid test results for COVID-19 and chest CT manifestation may help distinguish COVID-19 from non-COVID-19 cases.
Data Availability
Data Availability The data used to support the findings of this study are available from the corresponding author upon request.
Data Availability
The data used to support the findings of this study are available from the corresponding author upon request.
Ethics approval and consent to participate
The clinical research ethics boards of the West China Hospital approved the study, ethics code: 2019(130).
Conflicts of Interest
The authors declare that there are no conflicts of interest associated with the publication of this paper.
Authors’ contributions
Xiao-Jin Li conceived and designed the study. Xiao-Jin Li and Bin-Xing Shuai retrieved the medical databases, screened the literature, and extracted the data. Zhong-Wei Zhang conducted quality evaluation and statistical analyses. Yan Kang contributed to validation project administration. The manuscript was drafted and examined by Xiao-Jin Li and Yan Kang. All authors read and approved the final manuscript.
Acknowledgements
This work was supported by the 1·3·5 Project for disciplines of excellence-clinical Research Incubation Project(2019HXFH061), West China Hospital, Sichuan University, and the Sichuan University Spark Project (2018SCUH0031). The authors thank Professor Xue-Lian Liao, statistician Cai-Rong Zhu and Jing Zhang for their contributions to this study.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}