
Abstract
Background The COVID-19 pandemic is spreading worldwide. Italy emerged early on as the country with the largest outbreak outside Asia. The outbreak in Northern Italy demonstrates that it is fundamental to contain the virus’ spread at a very early stage of diffusion. At later stages, no containment measure, even if strict, can prevent the saturation of the hospitals and of the intensive care units in any country.
Methods and Results Here we show that it is possible to predict when the intensive care units will saturate, within a few days from the first cases of COVID-19 intensive care patients. Using early counts of intensive care patients, we predict the saturation for Lombardy, Italy.
Conclusions Governments should use the Italian outbreak as a precedent and implement appropriate containment measures to prevent the saturation of their intensive care units and protect their population, also, and above all, in anticipation of a possible second rapid spread of infections.
Introduction
The Coronavirus Disease 2019 (COVID-19) is a respiratory infectious disease caused by SARS-CoV-2 (also known as 2019-nCoV), which originated in Wuhan, China, in early December 2019. On January 23rd, Wuhan city shut down public transportation and airways; one week later, Wuhan and other cities in the province of Hubei, imposed strict social distancing measures (closure of school and non-essential work activities), combined with active search and isolation of infective cases and their contacts; on February 13th, all non-essential companies and manufacturing plants were closed. On February 15th, France reported the first death from COVID-19 outside Asia, while dozens of countries document cases of infection. On February 24th, three weeks after the lockdown of Wuhan and other cities, cases in China have fallen from an average of 2,500 daily cases of two weeks before to 400 cases. In the meanwhile, Italy emerged as the country with the largest outbreak outside Asia. On March 9th, Italy imposed a lockdown of the whole nation. On March 11th, the World Health Organization (WHO) declared the pandemic state, with more than 118,000 cases in 114 countries. On March 19th, while China announced that the incidence was brought to negligible levels and attempts to prudently restart normal life were initiated, deaths outside China overtook those counted in China. On March 19th, Italy counted 3,405 deaths, surpassing China. In Europe, several countries experienced similar exponential growth of cases as Italy, with just a few days of delay (Fig. 1). Spain and France imposed a lockdown on March 14th and on March 17th, respectively. On March 21st, Italy imposed a full lockdown of the nation, closing all non-essential companies and manufacturing plants.

Trajectories are shifted temporally to superpose one on another, so that for all countries day zero represents the onset of COVID-19 outbreak. Japan and Singapore were able to contain the outbreak at a the very early stage. The Chinese region of Hubei was able to contain diffusion at a later stage, by imposing a lockdown of the population on January 30th 2020 (red triangle), and a full lockdown of the population on February 13th 2020 (red diamond), closing all non-essential companies and manufacturing plants. Italy, Spain, France, UK, and the American States of California and New York (referred as US*) display exponential growth of confirmed cases. Italy, Spain, France and US* imposed a lockdown at similar (relative) times, indicated by the green, gold, blue and purple triangle, respectively. The four countries have comparable population sizes to Hubei region, with a minimum of Spain (46.7M people) and a maximum of France (66.9M). Italy additionally imposed a full lockdown 12 days afterwards (green diamond).
China was able to control the outbreak of COVID-19 in about two months by implementing strong containments measures, such as lockdown of the population (1). Lockdown can appear as an extreme measure, but it is not. Mild restrictions, such closure of schools and partial closure of workplaces, can lower the basic reproduction number of infection (R0) but not below the unit. With mild restrictions, the number of infections would grow at the same rate for a period equal to the incubation time (which is below 14 days for 99% of COVID-19 infections (2)), and would then grow exponentially at a lower rate. Therefore, mild restrictions would slow down the epidemic, but not control it (3). In this work, we discuss the necessity and efficacy of lockdown measures for controlling the outbreak of COVID-19, analyzing data from Italy, the country with the largest recorded outbreak of the disease today.
COVID-19 represent a severe challenge for National Health Systems
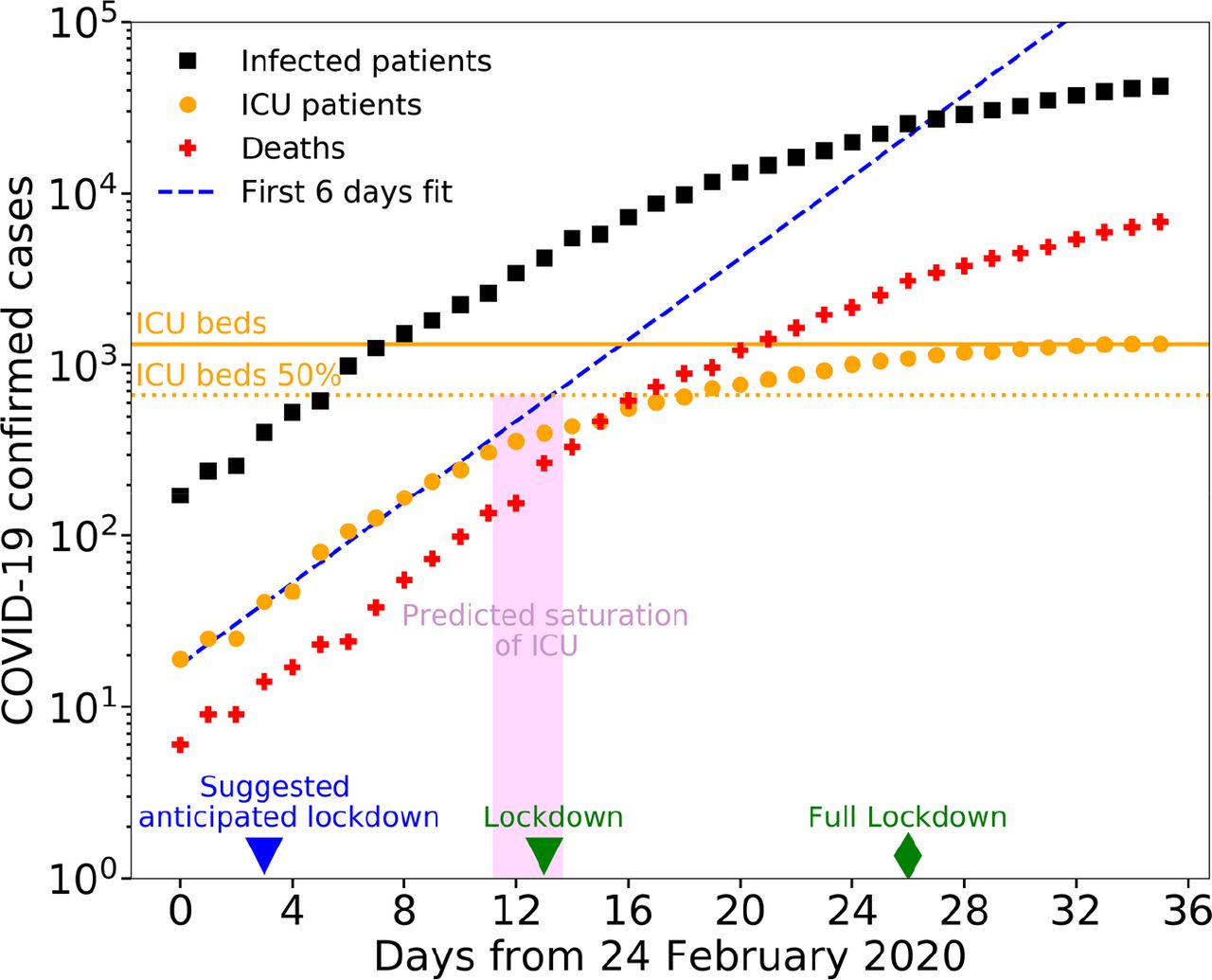
National Health Systems (NHS) face a major challenge from COVID-19 infection: the exponential increase of patients needing hospitalization in intensive care units (ICU). In Italy, the 2018-2019 seasonal influenza required 812 intensive care beds (4), while COVID-19 infection required more than 1000 ICU beds after just 21 days from the first detected cases on February 24th 2020 (Fig. 2).

The number of infected patients (black squares) and deaths (red crosses) increases exponentially in time (note that vertical axis has exponential units). Intensive care patients (orange circles) displays a deviation from the exponential growth: their growth is slower than exponential as their number reaches the capacity of the NHS (due to the saturation of the ICU beds in the Italian regions of Lombardy, Piedmont, Marche, Trentino Alto Adige, Valle d’Aosta, which host 28% of the Italian population). The green triangle and diamond represent the lockdown day (March 9th 2020) and full lockdown day (March 21st 2020). The orange solid line and dotted line represent 100% and 50% of the total number of ICU beds in Italy before the onset of the epidemic, which was equal to 5090 (5).
While NHS are prepared to receive a certain number of ICU patients distributed during the influenza season, which lasts several months, no NHS can manage an exponentially growing number of COVID-19 patients. To avoid the saturation of the ICUs, governments need to impose strong containment measures, such as lockdown of the population. Acting early is paramount: after containments measures are taken, the number of cases still grows exponentially for at least ten days, due to infections contracted before the measures (2). The later these containment measures are taken, the stronger these measures need to be to contain diffusion of COVID-19, and could be anyways insufficient to avoid the catastrophic collapse of the NHS. For example, Japan and Singapore were able to avoid a lockdown of the population, because the governments implemented a range of measures at a very early stage of the outbreak (Fig. 1).
COVID-19 epidemic in Italy can be used as a precedent for other countries
From the early stage of the COVID-19 outbreak (February 24th 2020), Italy is providing statistics of the epidemic, through a daily bulletin and an open-access repository (10). This repository contains daily counts of confirmed cases, hospitalized patients, ICU patients, and deceased patients, at the national and regional level (Fig. 3). This repository represents an important and unique source of information for other countries that the pandemic will reach. The number of ICU patients represents a more robust information compared to the number of infected people, which is subject to an under-reporting. The number of infected people strongly depends on the number of performed tests and on the strategy of sampling of the population (e.g. only symptomatic people, random people). Testing capability and strategy might largely vary among different countries, while ICU patients count is a routine operation performed by all NHSs. ICU counts are more reliable also compared to deaths counts, since most patients dying with COVID-19 have comorbidities and ascertaining that COVID-19 was the primary cause of death can be complicated. For example, Germany reported no cases of death due to SARS-CoV-2 until there were 1139 confirmed cases. Generally, ICU patients counts offers reliable information of the evolution of COVID-19 epidemic, at least until the ICU capability of the NHS is not yet saturated.

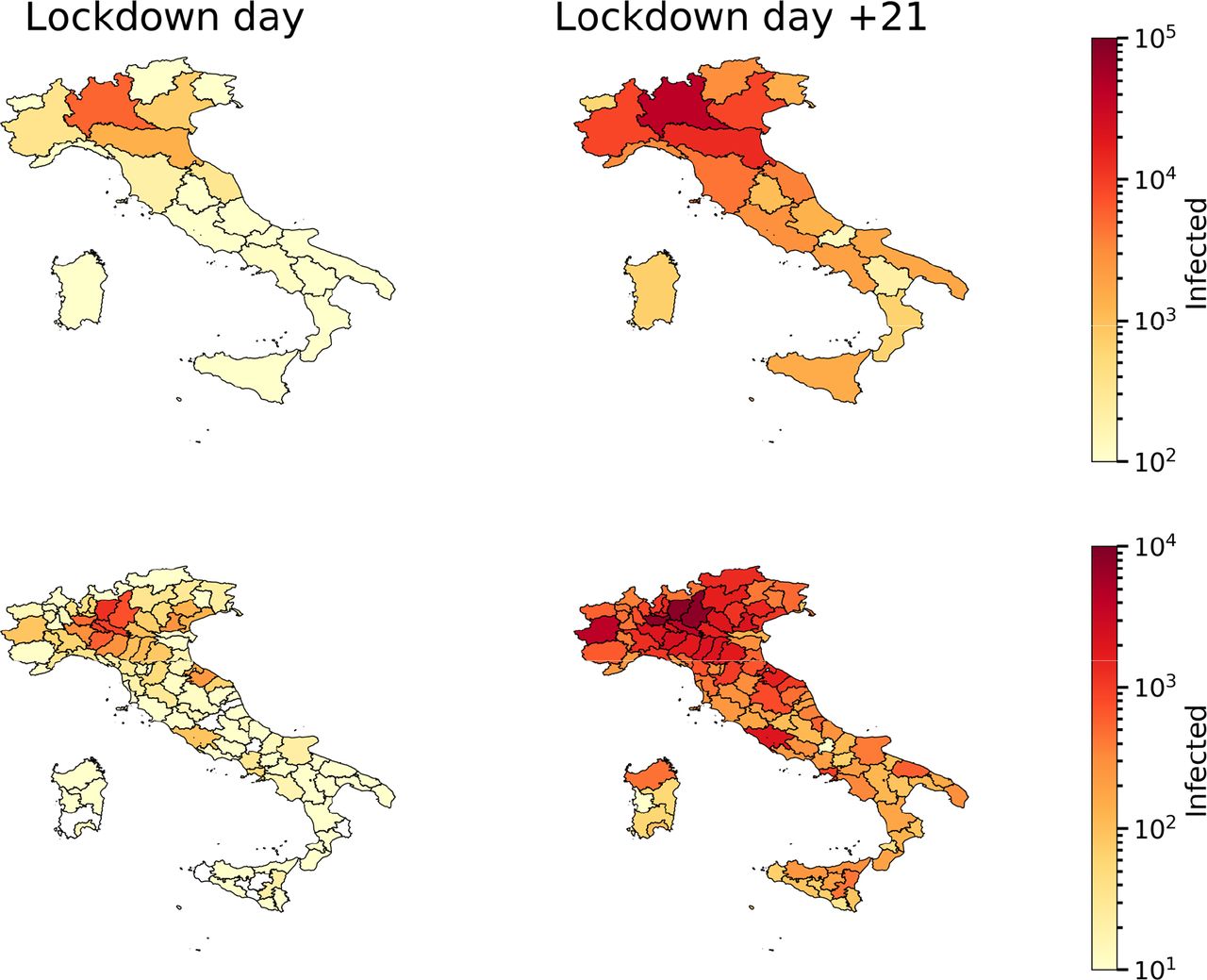
The maps on the left represent the number of infection cases detected at the regional level (top panel) and the provincial level (bottom panel), on March 9th, when lockdown was imposed. The maps on the right represent the number of total confirmed cases twenty-one days later, on March 30th.
COVID-19 cases evolution in Italy
COVID-19 outbreak in Italy started in Codogno, a town of 15,868 inhabitants in Lombardy region. After ten days from the first ICU patient (February, 20th 2020), the number of COVID-19 ICU patients was already larger than 100; after 18 days, ICU patients occupied about the 50% of the total ICU beds of Lombardy region. This percentage is close to the average percentage of ICU beds that are available during a whole year in Italy(5). At the early stage of the COVID-19 outbreak, the number of ICU beds in Italy was approximately 5090 (i.e. 8,42 ICU beds per 100.000 inhabitants (5)) and Lombardy region had approximately 900 ICU beds (9 ICU beds per 100.000 inhabitants). The Italian government immediately implemented several measures to increase the number of available ICU beds, for example postponing non-essential surgical operations and purchasing mechanical ventilators for new ICUs, and to increase medical support, for example by recalling retired doctors. Yet, these measures offer what we call a linear response, which is not sufficient to face an exponential growth of ICU beds demand.
The Italian government implemented also a series of measures to slow down the diffusion of the virus. Schools and universities were closed in Lombardy on February 26th, and in rest of Italy on March 5th. On March 8th, Lombardy region ordered a lockdown of the populations (Decreto del Presidente del Consiglio dei Ministri 8 Marzo 2020). On the following day, the lockdown was extended to the entire nation. In Lombardy and in Italy, nurses, doctors and health-care professionals have fought with incredible strength, acting as war heroes in dark times. However, the ICUs rapidly saturated by COVID-19 ICU patients in Lombardy region (Fig. 4) and subsequently in other regions (Fig. 5). On March 21st, the Italian government imposed a full lockdown of the nation, closing off all the non-essential companies and manufacturing plants.

The number of deaths (red crosses) grows exponentially in time in Lombardy region, Italy. The number of ICU patients (orange circles) shows a flattening trend in time. The slower growth of ICU patients indicates the saturation of the ICU beds in the region. The dotted blue line is the linear regression of the first six orange datapoints. The day of saturation can be predicted by linear regression, fitting the logarithm of the number of ICU patients, at early stages of the epidemic: the magenta rectangle shows the predicted temporal range for the saturation of 50% of the ICU beds; the extremes of the range are obtained by fitting the first four (blue triangle) and nine orange datapoints. To avoid incurring in the ICUs saturation, an anticipated lockdown would have been necessary, as indicated by the blue triangle. The green triangle and green diamond represent the lockdown day (March 8th 2020) and full lockdown day (March 21st 2020). The orange solid line and dotted line represent 100% and 50% of the actual total number of ICU beds in Lombardy.

The maps represent the ICUs saturation (number of ICU patients divided by number of ICU beds) at the regional level on March 9th (left panel), when lockdown was imposed, and twenty-one days later, on March 30th (right panel). Here we use the regional number of ICU beds reported before the onset of the epidemic. This number has been increased during the epidemic.
Saturation of ICU can be predicted accurately early on
Here we show that it is possible to predict the date of saturation of the ICUs in a region early on, by using the temporal information about the number of available ICU beds. We focus on Lombardy region. The number of ICU patients in the region grew exponentially for the first ten days, starting from February 24th, and then slowed down as it reached the number of available ICU beds. We can predict the date at which the ICU beds became saturated by performing a linear regression of the logarithm of the number of ICU patients, starting from the first four datapoints (Fig. 4). This result shows that monitoring the ICUs statistics at the beginning of the epidemic allows countries to assess the date of possible saturation of the ICU beds early on. Monitoring the ICUs early in the outbreak is paramount: Lombardy in Italy has one the best NHS in the World (6,7), therefore most countries will face the saturation of their ICU beds at earlier stages of the outbreak. It is worth to note that several factors can affect the time to saturate the ICU beds. In particular, the saturation time depends on the connectivity of the population: the more people are connected within a region, the faster the infection diffuses (8). Therefore, the risk of ICUs saturation is higher for the most developed and connected regions, and Lombardy is the most connected region of Italy. Moreover, if a lock down measure is imposed, the saturation time depends on the incubation time of the disease and on the degree of adherence of the population to the lockdown.
Lockdown benefits for Italy
Here we analyze the effects of the lockdown of the Italian population. Italy imposed two major containment measures: the lockdown on March 9th 2020, and a full lockdown on March 21st 2020, where all non-essential companies and manufacturing plant were closed. These measured helped to avoid the collapse of the whole national health system, yet they could not avoid the saturation of the ICU beds in several Italian regions (Fig. 5).
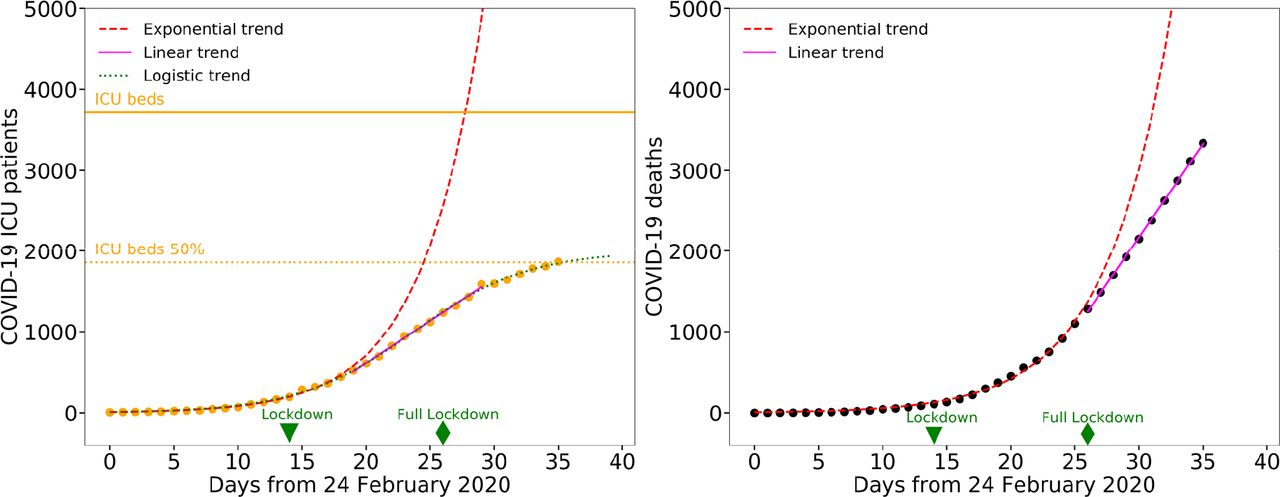
The effects of the confinement measures become evident with some delay. Specifically, we expect the effect on the number of ICU patients to appear within about two weeks (i.e. the maximum incubation time), and on the number of deaths to appear in about three weeks (i.e. the time from infection to death) (2). At the current moment, 21 days have passed from the national lockdown, so we expect to see effects on both the number of ICU patients and deaths. Because of the saturation of the ICUs in several Italian regions, the number of ICU patients in Italy currently underestimates the number of cases that would require intensive care. Therefore, we analyze the data of Italy excluding the regions where the ICUs have saturated. This leaves us with 15 of the 20 regions and excludes about 28% of the Italian population. We find that the recent growth of ICU patients and deaths is consistent with a linear growth, rather than an exponential growth, suggesting that the lockdown measures have effectively reduced the spread of the infection (Fig. 6), as it has been for Hubei region (1). Specifically, for the number of ICU patients, we obtain a good fit using an exponential curve (ICU patients(t) ∝ exp[r t], t = days) up to five days after the lockdown (equal to the median incubation time of COVID-19 (9)), and a line (ICU patients(t) ∝ b t, t = days) for later datapoints, up to fifteen days after the lockdown. We suggest that a logistic curve might represent well the overall trend of ICU patients in time (Fig. 6a). For the number of deaths in time, we obtain a good fit using an exponential curve up to eleven days after the lockdown, and a line for later datapoints (Fig. 6b).

a, The number of ICU patients grows slower than exponential starting from March 14th, i.e. five days after the lockdown of March 9th (green triangle). Five days correspond to the current estimate of median incubation time of COVID-19 (9). We divided the datapoints into two groups, before March 14th and between March 14th and March 24th, and we fit the first group with an exponential curve (red dashed line, ICU patients(t) ∝ exp[r t], t = days), and the second group with a line (magenta line, ICU patients(t) ∝ b t, t = days). The best fit parameters are r = 0.213 (95 % CI : 0.205 – 0.221), and b = 104 (95 % CI : 102 – 106). The root mean square error (RMSE) and normalized-RMSE (n-RMSE) of the exponential fit are 13.80 and 3.1 %, respectively. RMSE and n-RMSE for the linear fit are 18.73 and 1.8 %, respectively. The green dashed line is the overall best fit logistic curve. b, As for panel a, representing the number of deaths. The linear trend starts eleven days after the lockdown. The best fit parameters are r = 0.197 (95 % CI : 0.193 – 0.201), and b = 230 (95 % CI : 228 – 232). RMSE and n-RMSE for the exponential fit are 20.57 and 1.9 %, respectively; RMSE and n-RMSE for the linear fit are 18.84 and 0.9 %, respectively. For both panels, we excluded from the analysis the Italian regions where the ICUs saturated, i.e. Lombardy, Piedmont, Marche, Trentino Alto Adige, Valle d’Aosta, which host 28% of the total Italian population. The non-linear least squares problems have been solved using Levenberg-Marquardt algorithm, with NumPy library (Python).
Overall, this analysis suggests that 21 days after the lockdown of the Italian population, the growth of ICU patients and deaths is slower than exponential. This implies that the lockdown has spared thousands of lives. At the time we write this manuscript, we cannot offer a good estimate of the number of lives that were spared, as we cannot yet fit a logistic curve to the number of deaths reliably.
Conclusions
In this work, we analyzed the temporal evolution of COVID-19 outbreak in Italy up to March 30th 2020 and we discussed the effects of the national lockdown in containing the diffusion. The saturation of the ICUs in many Italian regions suggests that containment measures were taken too late. Using Italy as a precedent, other countries should impose these confinement measures at earlier stages of the outbreak to be able to protect their population from COVID-19. We show that countries can predict the date of saturation of their ICUs early on, as soon as an exponential growth of intensive care patients is observed, as it was in Lombardy region. The Italian case demonstrates that a national lockdown is effective in reducing the growth of ICU patients. The saturation of ICUs, thus the collapse of a NHS, would be a catastrophe affecting the entire population of a nation. People would die if they needed intensive care for any reason, no matter their age or their wealth. The saturation of the Italian intensive care units suggests that other governments should act early to contain CODIV-19 and consider stronger measures than lockdown, including immediate closing of non-essential companies and manufacturing plants. These results can help design better policies to contain a possible second rapid spread of infections, such as the one that already occurred in Hong Kong after the relaxation of the first containment measures.
We strongly encourage any government to accurately share data, including ICU patients; this data will significantly help the understanding of present and future evolution of the COVID-19 pandemic. Italy has been the first country in Europe in which the pandemic outbreak has been observed, and it has adopted a politic of wide dissemination of open data with detailed spatial structure. Unprecedented measures have been taken by the Italian government, including systematic sharing of ICUs information, and lockdown of the country. Most likely, the decisions taken in Italy between February 24th and March 21st have saved thousands of lives, not only within national borders.
Data Availability
The Italian COVID-19 data are available through a GitHub repository managed by the DPC (Dipartimento della Protezione Civile - Presidenza del Consiglio dei Ministri). For Figure 1, we used World COVID-19 data published by the EU agency for Disease Prevention and Control. For Figure 1, we also used the dataset maintained by the Center for Systems Science and Engineering (CSSE) at Johns Hopkins University (JHU), for the time series of the Chinese Hubei region. For Figure 1, we finally used the dataset maintained by the New York Times, for the time series of the US* (New York State + California State). The number of available beds in ICU in Italy before the onset of the epidemic have been extracted from the dataset published by the Italian Ministry of Health.
https://github.com/pcm-dpc/COVID-19.
https://github.com/CSSEGISandData/COVID-19
https://github.com/nytimes/covid-19-data
http://www.dati.salute.gov.it/imgs/C_17_dataset_17_0_upFile.csv
Authors’ contributions
MS analyzed the data, conceived the manuscript and, together with FL, prepared the figures. All the authors contributed to the interpretation of the data and the discussion of the results. MS and ADC wrote the manuscript, and all the authors reviewed it.
Competing interests
The authors declare that they have no competing interests.
Availability of data and materials
The Italian COVID-19 data are available through a GitHub repository managed by the DPC (Dipartimento della Protezione Civile - Presidenza del Consiglio dei Ministri): https://github.com/pcm-dpc/COVID-19
For Figure 1, we used World COVID-19 data published by the EU agency for Disease Prevention and Control: https://www.ecdc.europa.eu/en/publications-data/download-todays-data-geographic-distribution-covid-19-cases-worldwide
For Figure 1, we also used the dataset maintained by the Center for Systems Science and Engineering (CSSE) at Johns Hopkins University (JHU), for the time series of the Chinese Hubei region: https://github.com/CSSEGISandData/COVID-19
For Figure 1, we finally used the dataset maintained by the New York Times, for the time series of the US* (New York State + California State): https://github.com/nytimes/covid-19-data
The number of available beds in ICU in Italy before the onset of the epidemic have been extracted from the dataset published by the Italian Ministry of Health: http://www.dati.salute.gov.it/imgs/C_17_dataset_17_0_upFile.csv
Acknowledgments
This manuscript has been written with the hope that the heroic resistance showed by the city of Bergamo, the Lombardy region and the whole of Italy will not be needed elsewhere.
The authors want to thank all the Italian nurses, doctors and health-care professionals that are fighting against an invisible enemy as war heroes in dark times. This manuscript is dedicated to the memory of Doctor Li Wenliang, who first tried to warn the World about COVID-19, and all the health-care professionals who died fighting against this virus.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}