
Abstract
Introduction SARS-Cov-2 (severe acute respiratory disease coronavirus 2), which causes Coronavirus Disease 2019 (COVID19) was first detected in China in late 2019 and has since then caused a global pandemic. While molecular assays to directly detect the viral genetic material are available for the diagnosis of acute infection, we currently lack serological assays suitable to specifically detect SARS-CoV-2 antibodies.
Methods Here we describe serological enzyme-linked immunosorbent assays (ELISA) that we developed using recombinant antigens derived from the spike protein of SARS-CoV-2. These assays were developed with negative control samples representing pre-COVID 19 background immunity in the general population and samples from COVID19 patients.
Results The assays are sensitive and specific, allowing for screening and identification of COVID19 seroconverters using human plasma/serum as early as 3 days post symptom onset. Importantly, these assays do not require handling of infectious virus, can be adjusted to detect different antibody types and are amendable to scaling.
Conclusion Serological assays are of critical importance to determine seroprevalence in a given population, define previous exposure and identify highly reactive human donors for the generation of convalescent serum as therapeutic. Sensitive and specific identification of Coronavirus SARS-Cov-2 antibody titers will also support screening of health care workers to identify those who are already immune and can be deployed to care for infected patients minimizing the risk of viral spread to colleagues and other patients.
Introduction
On December 31st, 2019 China reported first cases of atypical pneumonia in Wuhan, the capital of Hubei province. The causative virus was found to be a betacoronavirus, closely related to the severe acute respiratory syndrome coronavirus (SARS-CoV-1) from 2003 and similar to Sarbecoviruses isolated from bats.1,2 It was therefore termed SARS-CoV-2 and the disease it causes was named COVID19 (COronaVIrus Disease 2019).3 The outbreak in Wuhan expanded quickly and led to the lockdown of Wuhan, the Hubei province and other parts of China. While the lockdown, at least temporarily, brought the situation under control in China, SARS-CoV-2 spread globally causing a pandemic with, so far, 150,000 infections and 5,500 fatalities (as of March 16th, 2020).
Nucleic acid tests that detect the SARS-CoV-2 RNA genome were quickly developed and are now widely employed to diagnose COVID19 disease.4,5 However, there remains a great need for laboratory assays that measure antibody responses and determine seroconversion. While such serological assays are not well suited to detect acute infections, they are support a number of highly relevant applications. First, serological assays allow us to study the immune response(s) to SARS-CoV-2 in dynamic qualitative and quantitative manner. Second, serosurveys are needed to determine the precise rate of infection in an affected area, which is an essential variable to accurately determine the infection fatality rate. Third, serological assays will allow for the identification of individuals who mounted strong antibody responses and who could serve as donors for the generation of convalescent serum therapeutics. Lastly, serological assays will permit to determine who is immune and who is not. This would be very useful for deploying immune healthcare workers in a strategic manner as to limit the risk of exposure and spread of the virus inadvertently.
Sarbecoviruses express a large (approximately 140 kDa) glycoprotein termed spike protein (S, a homotrimer), which mediates binding to host cells via interactions with the human receptor angiotensin converting enzyme 2 (ACE2).6-8 The S protein is very immunogenic with the receptor-binding domain (RBD) being the target of many neutralizing antibodies.9 Individuals infected with coronaviruses typically mount neutralizing antibodies, which might be associated with some level of protection for a period of months to years, and neutralizing response has demonstrated for SARS-CoV-2 in an individual case from day 9 onwards.10-13 Serum neutralization can be measured using live virus but the process requires several days and must be conducted under biosafety level 3 laboratory containment for SARS-CoV-2 Potentially, pseudotyped viral particle entry assays based on lentiviruses or vesicular stomatitis virus can be used as well, but these reagents are not trivial to produce. A simple solution is the use of a binding assay, e.g. an enzyme linked immunosorbent assays (ELISA), with recombinantly expressed antigen as substrate. Here we report the development of such an assay and provide a protocol for both recombinant antigen production as well as the ELISA.
Results
Expression constructs and generation of recombinant SARS-Cov-2 proteins
We generated two different versions of the spike protein. The first construct expresses a full length trimeric and stabilized version of the spike protein and the second only the much smaller receptor binding domain (RBD). The sequence used for both proteins is based on the genomic sequence of the first virus isolate, Wuhan-Hu-1, which was released on January 10th 2020.1 Sequences were codon optimized for mammalian cell expression. The full-length spike protein sequence was modified to remove the polybasic cleavage site, which is recognized by furin and to add a pair of stabilizing mutations (Figure 1).7,14,15 These two modifications were included to enhance the stability of the protein based on published literature.7,14 At amino acid P1213 the sequence was fused to a thrombin cleavage site, a T4 foldon sequence for proper trimerization and a C-terminal hexahistidine tag for purification (Figure 1).16,17 The sequence was cloned into a pCAGGS vector for expression in mammalian cells and into a modified pFastBac Dual vector for generation of baculoviruses and expression in insect cells. For expression of the RBD, the natural N-terminal signal peptide of S was fused to the RBD sequence (amino acid 419 to 541) and joined with a C-terminal hexahistidine tag.18 The same vectors as for the full length S protein were used to express the RBD. In mammalian cells, the RBD domain gave outstanding yields (approximately 25 mg/liter culture), but expression was lower in insect cells (approximately 0.4 mg/liter culture). Clear single bands were visible when the recombinant RBD proteins were analyzed on a reducing sodium dodecyl sulfate–polyacrylamide gel electrophoresis (SDS-PAGE), with the insect cell derived protein (iRBD) running slightly lower than the mammalian cell derived protein (mRBD) (Figure 1). The size difference likely reflects differences in glycan sizes between insect cells and mammalian cells. The full-length S protein was expressed in both systems with slightly higher yields in mammalian cells (mSpike) than in insect cells (iSpike) (approximately 2 mg/liter cultures versus 0.5 mg/liter culture). The full-length protein appeared as a double band on a reducing SDS-PAGE, the higher species likely being the full-length protein and the slightly lower species likely a cleavage product.

A Visualization of the trimeric spike protein of SARS-CoV-2 based on PBD # 6VXX using Pymol.8 One monomer is colored in dark blue while the remaining two monomers are held in light blue. The receptor binding domain (RBD) of the dark blue trimer is highlighted in red. B Schematic of the wild type full length spike protein with signal peptide, ectodomain, receptor binding domain, furin cleavage site, S1, S2, and transmembrane and endodomain domain indicated. C Schematic of the soluble trimeric spike. The polybasic/furin cleavage site (RRAR) was replaced by a single A. The transmembrane and endodomain were replaced by a furin cleavage site, a T4 foldon tetramerization domain and a hexahistidine tag. Introduction of K986P and V987P has been shown to stabilize the trimer in the pre-fusion conformation. D Schematic of the soluble receptor binding domain construct. All constructs are to scale. E Reducing SDS PAGE of insect cell and mammalian cell derived soluble trimerized spike protein (iSpike and rSpike). F Reducing SDS PAGE of insect cell derived and mammalian cell derived recombinant receptor binding domain (iRBD and mRBD).
ELISA development
We used a panel of 59 banked human serum samples collected from study participants including participants with confirmed previous viral infections (e.g., hantavirus, dengue virus, coronavirus NL63 – sample take 30 days post symptom onset) to establish an ELISA with these proteins. These human sera were used to test the background reactivity to the SARS-CoV-2 spike in the general US population covering an age range from approximately 20 to 65+ years. Four plasma/serum samples from three COVID19 patients were used to determine the reactivity of SARS-CoV-2 infected individuals to the RBD and the full length spike.
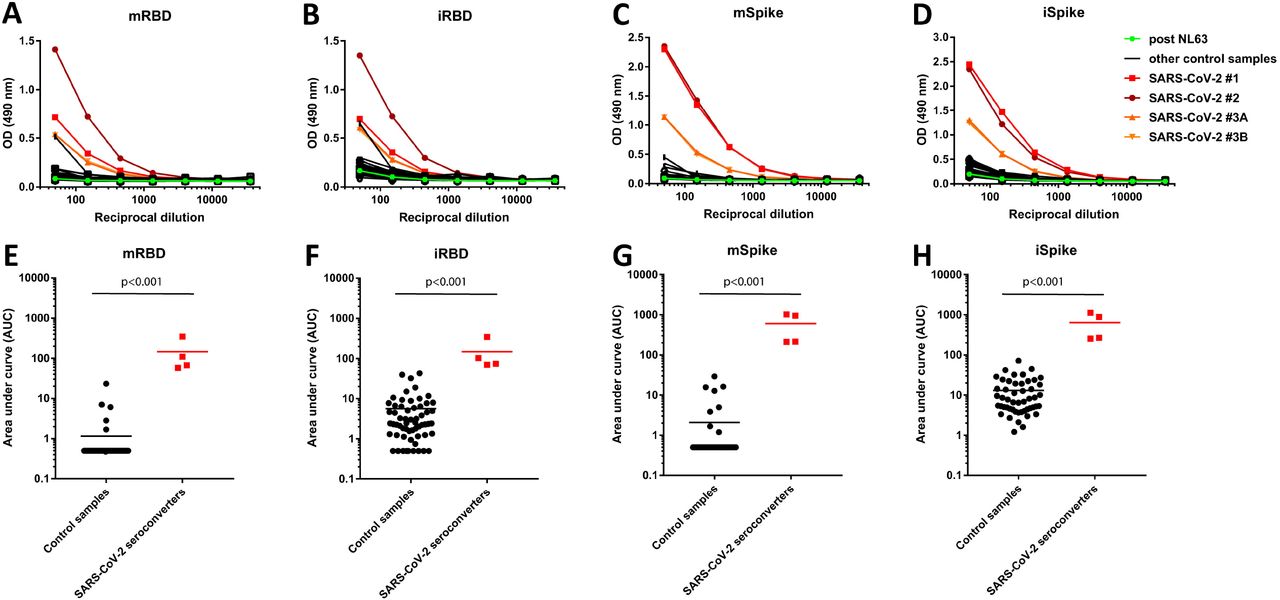
ELISAs were performed by doing serial dilution of the individual serum samples. Values from the dilution curves were used to determine the area under the curve (AUC), which was graphed. All COVID10 plasma/serum samples reacted strongly to both RBD and full-length spike protein while reactivity of the other serum samples only yielded background reactivity (Figure 2). Reactivity of COVID19 sera was, in general, stronger against the full-length S protein than against the RBD, likely reflecting the higher number of epitopes found on the much larger spike protein. For the RBD the difference between control sera and convalescent sera was larger when the insect cell derived protein was used as compared to the mammalian cell derived RBD. The same was true for the full-length spike protein. The assay allowed to clearly distinguish the convalescent sera from the banked control sera.

A-D Reactivity to insect cell derived RBD (iRBD), mammalian cell derived RBD (mRBD), insect cell derived soluble spike protein (iSpike) and mammalian cell derived soluble spike protein (sSpike). Sera from three SARS-CoV-2 infected individuals were used and are shown in shades of red. Two samples are from the same patient but from different time points (SARS-CoV-2 #3A and #3B). One sample, shown in green, is a convalescent serum sample post NL63 infection. E-F shows data from the same experiment but graphed as area under the curve (AUC) to get a better quantitative impression. The n for the control samples is 50 except for the iRBD were it is 59. Statistics were performed using a student’s t-test in Graphpad Prism.
Antibody isotyping and subtyping
For the four COVID19 patient plasma/sera, we also performed an isotyping and subtyping ELISA using the insect cell and mammalian cell expressed S proteins. Strong reactivity was found for all samples for IgG3, IgM and IgA (Figure 3). An IgG1 signal was also detected for three out of the four samples, while one sample showed no reactivity. No signal was detected for IgG4 and reagents for IgG2 were unavailable.

Insect cell derived (A) and mammalian cell derived (B) spike protein was used to study isotype/subclass distribution of antibodies. The different samples are indicated by different symbols. Sera from three SARS-CoV-2 infected individuals were used and are shown in shades of red. Two samples are from the same patient but from different time points (SARS-CoV-2 #3A and #3B).
Discussion
Here we describe a serological method to detect seroconversion upon SARS-CoV-2 infection. The method is based on reactivity to the immunogenic S protein of the virus. It is relatively simple and quick in its execution and can be performed at biosafety level 2 level as it does not involve life virus. We have tested these methods using banked serum samples obtained from study participants in 2019 and early 2020 when this virus was not widely circulating in the US. These serum samples produced low, close to baseline signals in our ELISA. Since the age range of the participants was broad, ranging from to 65+ years of age, it is likely that most had experienced infections with human coronaviruses including the alphacoronaviruses NL63 and 229E as well as the betacoronaviruses OC43 and HKU1. We included paired serum samples (acute and convalescent) from a participant with a laboratory confirmed coronvirus NL63 infection. Our data show that there is no or only negligible cross-reactivity from human coronaviruses to SARS-CoV-2. Of note, even infection with the human alphacoronavirus NL63, which also uses ACE2 as receptor19, did not induce cross-reactivity. This is of great importance because it suggests that humans are completely naïve to SARS-CoV-2, which may explain the relatively high R0 of SARS-CoV-2 compared to other respiratory viruses such as influenza virus.20 It might also suggest that antibody-dependent enhancement from human coronavirus induced cross-reactive antibodies targeted at the S protein is unlikely to be the cause of the high pathogenicity of the virus in humans.21
The plasma/sera used in this study from patients with COVID19 were obtained at day 20 (SARS-CoV2 #1), at day 4 (SARS-CoV-2 #2), days 2 and 6 (SARS-CoV-2 #3A and B) post symptom onset. Our data shows significant seroconversion after natural infection with SARS-CoV-2. Our results suggest that antibodies mounted upon infection target the full length S protein as well as the RBD, which is the major target for neutralizing antibodies for related viruses coronaviruses.9 In fact, sample SARS-CoV2 #1 was tested in another study in neutralization assays and showed a neutralizing titer of 1:160.13 Thus, seroconversion may lead to protection at a minimum for a limited time. Interestingly, the IgG3 response was stronger than the IgG1 response which is in contrast to e.g. the immune response to influenza where usually IgG1 responses dominates.22,23 Lastly, we also detected strong IgA and IgM responses in the blood compartment. Of note, level of reactivity and antibody isotypes matched expected patterns based on time since symptom onset very well.
We believe that our ELISA method will be key for serosurveys aimed at determining the real attack rate and infection fatality rate in different human populations and to map the kinetics of the antibody response to SARS-CoV-2. In addition, clinical trials with convalescent serum as therapeutic have been initiated in China (e.g. NCT04264858) and anecdotal evidence from the epidemic in Wuhan suggests that compassionate use of these interventions was successful. China has recently shipped convalescent sera to Italy for use in patients and efforts to produce convalescent serum batches are ongoing in the US as well. Screening sera using our assay would be faster and easier than performing standard neutralization assays in BSL3 containment laboratories. Patients recovering from COVID19 disease could be screened for strong antibody responses using the assays described here, especially the one using the RBD as substrate since anti-RBD antibodies likely correlate with virus neutralization. In addition, the assay could be used to screen health care workers to allow selective deployment of immune medical personnel to care for patients with COVID19. Such a strategy would likely limit nosocomial spread of the virus. Of course, the generated recombinant proteins are also excellent reagents for vaccine development and can serve as baits for sorting B cells for monoclonal antibody generation. We are making the methods and laboratory reagents widely available to the research community in order to support the global effort to limit and mitigate spread of SARS-CoV-2.
Methods
Recombinant proteins
The mammalian cell codon optimized nucleotide sequence coding for the spike protein of SARS-CoV-2 isolate (GenBank: MN908947.3) was synthesized commercially (GeneWiz). The receptor binding domain (RBD, amino acid 319 to 541, RVQP….CVNF) along with the signal peptide (amino acid 1-14, MFIF….TSGS) plus a hexahisitidine tag was cloned into mammalian expression vector pCAGGS as well as in a modified pFastBacDual vectors for expression in baculovirus system. The soluble version of the spike protein (amino acids 1-1213, MFIF….IKWP) including a C-terminal thrombin cleavage site, T4 foldon trimerization domain and hexahistidine tag was also cloned into pCAGGS. The protein sequence was modified to remove the polybasic cleavage site (RRAR to A) and two stabilizing mutations were introduced as well (K986P and V987P, wild type numbering). Recombinant proteins were produced using the well-established baculovirus expression system and this system has been published in great detail in 16,24,25 including a video guide. Recombinant proteins were also produced in Expi293F cells (ThermoFisher) by transfections of these cells with purified DNA using ExpiFectamine 293 Transfection Kit (ThermoFisher). Supernatants from transfected cells were harvested on day 3 post-transfection by centrifugation of the culture at 4000 g for 20 minutes. Supernatant was then incubated with 6 mls Ni-NTA agarose (Qiagen) for 1-2 hours at room temperature. Next, gravity flow columns were used to collect the Ni-NTA agarose and the protein was eluted. Each protein was concentrated in Amicon centrifugal units (EMD Millipore) and re-suspended in phosphate buffered saline (PBS). Proteins were analyzed on reducing SDS-PAGE. The DNA sequence for all constructs is available from the Krammer laboratory. Several of the expression plasmids and proteins have also been submitted to BEI Resources and can be requested from their web page for free (https://www.beiresources.org/).
SDS-PAGE
Recombinant proteins were analyzed via a standard SDS-PAGE gel to check protein integrity. One ug of protein was mixed with 2X Laemmli buffer containing 5% beta-mercaptoethanol (BME) at a ratio of 1:1. Samples were heated at 100 °Celsius for 15 minutes and then loaded onto a polyacrylamide gel (5% to 20% gradient; Bio-Rad). Gels were stained with SimplyBlue SafeStain (Invitrogen) for 1-2 hours and then de-stained in distilled water overnight.
Human samples
Banked human samples were collected from study participants enrolled in ongoing IRB approved longitudinal observational study protocols of the Mount Sinai Personalized Virology Initiative. Samples were selected based on the date of collection (2019, early 2020) and whether participants had a documented history of viral infection. Samples were collected in the Clinical Research Unit at the Icahn School of Medicine at Mount Sinai after obtaining written consent and all participants agreed to sample banking and future research use. Self-reported ethnicities of the individuals from which samples were tested included Caucasian, Asian, African American and Hispanic. Samples included sera from a participant with acute NL63 infection as determined by the Biofire Respiratory panel. We included serum collected at day 3 post symptom onset as well as convalescent serum from the same person (day 30 post symptom onset). In addition, we tested convalescent sera from individuals with dengue, chikungunya and hantavirus infections. These samples served as negative controls given that they were collect prior to SARS-Cov-2 spread in the US. Six subjects were 20-29, 19 were 30-39, 13 were 40-49, 7 were 50-59 years old and six were 60 or older. For the mRBD ELISAs sera from additional nine t subjects were tested (30-39: 2; 40-49: 4; 50-59: 2; 60+: 1).
De-identified samples from the University of Melbourne and University of Helsinki were used as positive controls. For those, human experimental work was conducted according to the Declaration of Helsinki Principles and according to the Australian National Health and Medical Research Council Code of Practice. All participants provided written informed consent prior to the study. The studies were approved by the Alfred Hospital (ID #280/14) and University of Melbourne (ID #1442952.1, 1955465.2) Human Research Ethics Committees, and under research permit for project TYH2018322 of Helsinki University Hospital Laboratory.
ELISA
The ELISA protocol was adapted from previously established protocols 26,27. Ninety-six well plates (Immulon 4 HBX; Thermo Scientific) were coated overnight at 4°Celsius with 50 ul per well of a 2 ug/ml solution of each respective protein suspended in PBS (Gibco). The next morning, the coating solution was removed and 100 ul per well of 3% non-fat milk prepared in PBS with 0.1% Tween 20 (TPBS) was added to the plates at room temperature (RT) for 1 hour as blocking solution. Serum samples were heated at 56°C for 1 hour before use to reduce risk from any potential residual virus in serum. Serial dilutions of serum and antibody samples were prepared in 1% non-fat milk prepared in TPBS. The blocking solution was removed and 100 ul of each serial dilution was added to the plates for 2 hours at RT. Next, the plates were washed thrice with 250ul per well of 0.1% TPBS. Next, a 1:3000 dilution of goat anti-human IgG-horseradish peroxidase (HRP) conjugated secondary antibody (ThermoFisher Scientific) was prepared in 0.1% TPBS and 100 ul of this secondary antibody was added to each well for 1 hour. Plates were again washed thrice with 0.1% TBS. Once completely dry, 100 ul of SigmaFast OPD (o-phenylenediamine dihydrochloride; Sigma-Aldrich) solution was added to each well. This substrate was left on the plates for 10 minutes and then the reaction was stopped by addition of 50 μL per well of 3 M hydrochloric acid (HCl). The optical density at 490 nanometers was measured via a Synergy 4 (BioTek) plate reader. The background value was set at and optical density 490nm of 0.11 and area under the curve (AUC) was calculated. AUC values below 1 were assigned a value of 0.5 for graphing and calculation purposes. Data was analyzed in Prism 7 (Graphpad).
To assess the distribution of the different antibody isotypes/subclasses in the samples that reacted well in our standard ELISA, another ELISA was performed with different secondary antibodies 23. These antibodies include anti-human IgA (α-chain-specific) HRP antibody (Sigma A0295) (1:3,000), anti-human IgM (μ-chain-specific) HRP antibody (Sigma A6907) (1:3,000), anti-human IgG1 Fc-HRP (Southern Biotech 9054-05) (1:3,000), anti-human IgG3hinge-HRP (Southern Biotech 9210-05) (1:3,000), and anti-human IgG4 Fc-HRP (Southern Biotech 9200-05).
Data Availability
Data are available from the corresponding author.
Conflict of interest
The authors declare no conflict of interest.
Acknowledgements
We would like to thank Yong-Zhen Zhang (Fudan University) and Eddie Holmes (University of Sydney) for sharing the sequence of the first SARS-CoV-2 isolate in a very timely manner. We thank Jill Garlick and Janine Roney (Alfred Hospital, Melbourne) for data and specimen collection. We are also thankful to Genewiz for speeding up gene synthesis for this project, and being very accommodating to our needs. Furthermore, we want to thank Donna Tidmore for help with ordering primers with near light speed and and finally Susie (Changsu) Dong for commuting to New Jersey on several occasions to pick up reagents from Genewiz. We also thank the study participants for providing biospecimen for research purposes and the Conduits: Mount Sinai Health System Translational Science Hub (NIH grant U54TR001433) for supporting sample collection. The work of the Personalized Virology Initiative is supported by institutional funds and philanthropic donations. This work was partially supported by the NIAID Centers of Excellence for Influenza Research and Surveillance (CEIRS) contract HHSN272201400008C, the Australian National Health and Medical Research Council (NHMRC) NHMRC Program Grant (1071916) and NHMRC Research Fellowship Level B (#1102792), the Academy of Finland and Helsinki University Hospital Funds (TYH2018322). Finally, we want to thank the three COVID19 patients for their contribution to research and wish them a speedy recovery.





{kind=link}
{kind=link}
{kind=link}